
12th December 2023, NIA Diagnostic Imaging
One of the standout diagnoses I remember from medical school is renal artery stenosis. In practice, it is usually someone else that makes that diagnosis. It is not that uncommon. We may hear an abdominal bruit in our general vascular screen. We might struggle to get our patient’s BP to target despite the 4th or 5th agent. It might be a faster than normal deterioration of eGFR despite an improvement in BP control. Or worse, there are signs of heart failure in a younger patient. We think, maybe, there is RAS. Apart from referring to a specialist, how can we confirm the suspicion?
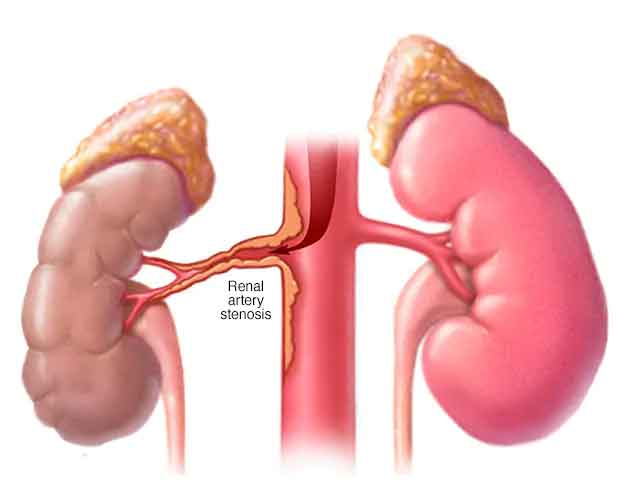
What is renal artery stenosis?
Atherosclerotic renal artery stenosis (ARAS) has become the leading cause of end stage renal disease in the elderly (12). The role of diagnostic imaging such as a CT renal angiogram in such patients is critical to ensure early detection of renal artery pathology and to guide appropriate treatment (12). Renal artery stenosis (RAS) is narrowing of one or more of the renal arteries (3), which progressively decreases blood flow to the kidneys (13). It is a major source of renovascular hypertension, which is the underlying cause in approximately 75% of the cases of secondary hypertension (10, 13).
Atherosclerosis, a condition characterised by the buildup of plaque within the arteries, is the most prevalent aetiology of RAS where ARAS, which primarily involves the proximal renal artery, accounts for 60-90% of all cases of RAS (3). Patients with RAS typically present with clinical characteristics of secondary hypertension which include hypertension that is severe, abrupt in onset, or resistant to treatment (14).
ARAS is a progressive disorder that can lead to worsening ct renal angiogram stenosis where 51% of patients reported worsening stenosis 5 years after diagnosis (14). It is associated with renovascular hypertension, ischemic nephropathy (8), decreased kidney function, chronic kidney disease and end-stage renal disease (3). Individuals with RAS are at an increased risk of cardiovascular events, with high cardiovascular morbidity and mortality rates (6). It was found that greater than 25% of all patients who die of cardiovascular disease have some degree of RAS (10). Thus, it is imperative to promptly diagnose and commence treatment as appropriate to achieve optimal patient outcomes.
What is a CT renal angiogram?
The most common imaging studies utilised to evaluate the presence of RAS are duplex ultrasonography, computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) (15).
A CT renal angiogram is a well-established minimally invasive diagnostic procedure for assessment of suspected RAS. This test involves the administration of intravenous contrast and acquiring detailed images to visualise the renal arteries, surrounding blood vessels and anatomical structures. This procedure is widely used for assessment of RAS because of its ease of availability, rapid acquisition, reproducibility, non-operator dependent and increased spatial resolution (12, 16). With high sensitivity (90% to 98%) and specificity (85% to 94%) in addition to aforementioned benefits (14), CT renal angiography is a valuable tool for diagnosing renal artery stenosis and can be performed in conjunction with a renal arterial doppler study.
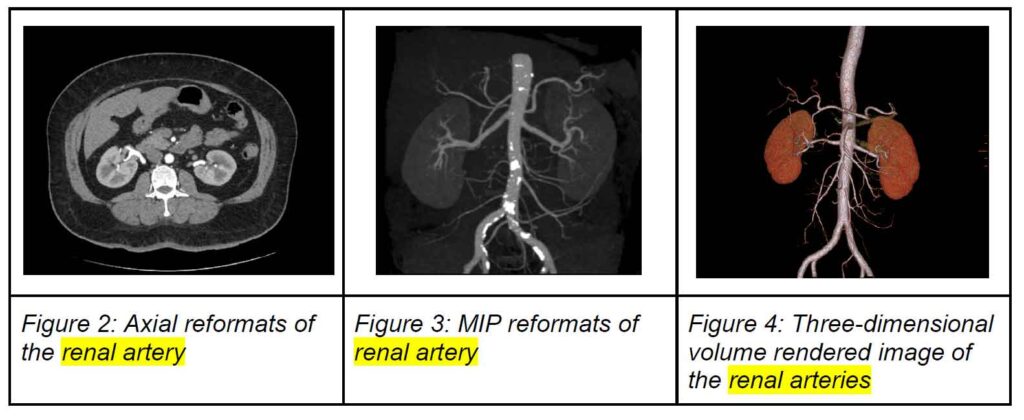
Following the examination, the axial source images are analysed on the GE Advantage Workstation to perform vessel analysis, and obtain multiplanar reconstructions (MPR), maximum intensity projection (MIP) images and three-dimensional volume rendered images.
What information does a CT renal angiogram provide?
CT renal angiography plays a significant role in the diagnosis of RAS, and provides
extensive information regarding its presence and extent:
● Visualisation of anatomical structures including the renal arteries: The generated reconstructed images and vascular detailing provides high-resolution images, enabling excellent visualisation of the renal arteries (both main and accessory), surrounding blood vessels and anatomical structures. This allows detection of any abnormalities, including stenosis, plaques or blockages (15, 16).
● Assessment of stenosis severity: Advancements in computer post-processing techniques allow various morphological measures of the renal vessels to be obtained from the quantitative data (1). Stenosis analysis can be performed to demonstrate the degree of narrowing in the renal arteries and determine the severity which is important for treatment planning and prognostication.
● Identification of atherosclerosis: As atherosclerosis is a common cause of RAS, CT renal angiography can reveal the presence of atherosclerotic plaques within the renal arteries and aid in diagnosis, and understanding of underlying pathology (8).
● Three-dimensional imaging: By post-processing volumetric data, a three-dimensional reconstruction of the renal vasculature can be rendered, offering a means to visualise the vascular tree (15). This is valuable for a comprehensive understanding of vascular anatomy, aiding in visualising the extent and location of stenosis.
● Evaluation of kidney perfusion and function: CT renal angiography allows for assessment of renal perfusion (blood flow) to the kidneys, helping determine the potential impact of RAS on kidney function and the overall clinical significance of the stenosis.
● Preoperative planning: In cases where surgical intervention is considered, such as renal artery angioplasty or stent placement, CT renal angiography provides detailed anatomical information of the specific location and characteristic of the stenosis, aiding in preoperative planning.
How is renal artery stenosis treated?
Diagnosis of RAS using imaging techniques such as CT renal angiography, is useful for guiding clinical decision making and appropriate therapy. Optimal medical therapy remains the central approach to treatment and management of RAS (15). Medications such as angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers (ARBs) can be prescribed (14). Other medications may be prescribed to manage comorbidities such as hypertension, hyperlipidaemia and diabetes as these conditions contribute to decline in renal function and accelerate the disease progression in ARAS (8). In addition, statins or antiplatelet therapy may be recommended.
For newly diagnosed ARAS, lifestyle modifications with diet, regular exercise and smoking cessation (8), can help manage contributing factors such as high blood pressure and atherosclerosis. Other procedures to treat RAS include surgical and percutaneous revascularisation (6), however, invasive management may only be indicated in a few cases such as symptomatic patients with severe RAS who continue to have acute severe worsening of renal function (14).
The ASTRAL trial was designed to determine whether there was clinical benefit from revascularisation adjunct to optimal medical therapy compared to medical therapy alone (2). It was found that revascularisation therapy was not associated with any benefit to renal function, blood pressure, renal or cardiovascular events, or overall mortality when compared with patients treated with antihypertensive, antiplatelet, and cholesterol-lowering medication alone (2, 14). However, a limitation of the study was that patients with severe RAS (those presenting with kidney injury or pulmonary oedema) were unlikely to be included in the trial, as they were likely treated with revascularisation immediately (14).
Conclusion
It is evident that CT renal angiogram is a valuable tool for diagnosing renal artery stenosis, and crucial in assisting with treatment pathways to ensure optimal patient outcomes. This scan can be performed at NIA Radiology at both sites in Glenquarie and Ingleburn.

REFERENCES
1. Andersson, M., Jägervall, K., Eriksson, P., Persson, A., Granerus, G., Wang, C., & Smedby, Ö. (2015). How to measure renal artery stenosis – a retrospective comparison of morphological measurement approaches in relation to hemodynamic significance. BMC Medical Imaging, 15, 42. https://doi.org/10.1186/s12880-015-0086-8
2. ASTRAL Investigators, Wheatley, K., Ives, N., Gray, R., Kalra, P. A., Moss, J. G., Baigent, C., Carr, S., Chalmers, N., Eadington, D., Hamilton, G., Lipkin, G., Nicholson, A., & Scoble, J. (2009). Revascularization versus medical therapy for renal-artery stenosis. The New England Journal of Medicine, 361(20), 1953–1962. https://doi.org/10.1056/NEJMoa0905368
3. Bokhari, M. R., & Bokhari, S. R. A. (2023, July 17). Renal Artery Stenosis. StatPearls Publishing. Retrieved December 1, 2023, from https://www.ncbi.nlm.nih.gov/books/NBK430718/
4. Cho, E. S., Yu, J. S., Ahn, J. H., Kim, J. H., Chung, J. J., Lee, H. K., & Lee, K. H. (2012). CT angiography of the renal arteries: comparison of lower-tube-voltage CTA with moderate-concentration iodinated contrast material and conventional CTA. American Journal of Roentgenology, 199(1), 96–102. https://doi.org/10.2214/AJR.11.7450
5. de Mello Júnior, C. F., Araujo Neto, S. A., de Carvalho Junior, A. M., Rebouças, R. B., Negromonte, G. R., & de Oliveira, C. D. (2016). Multidetector computed tomography angiography of the renal arteries: normal anatomy and its variations. Radiologia Brasileira, 49(3), 190–195. https://doi.org/10.1590/0100-3984.2014.0048
6. Gallagher, A., & Mangos, G. (2023). Renal artery stenosis and hypertension: when to screen and how to treat. Medicine Today, 24(3), 23-29. https://medicinetoday.com.au/mt/2023/march/feature-article/renal-artery-stenosis-and -hypertension-when-screen-and-how-treat#:~:text=Renal%20artery%20stenosis%20(RAS)%20is,warrant%20further%20investigations%20for%20RAS
7. John Hopkins Medicine. (n.d.). Resistant hypertension. Retrieved December 1, 2023, from https://www.hopkinsmedicine.org/health/conditions-and-diseases/high-blood-pressure-hypertension/resistant-hypertension#:~:text=Resistant%20hypertension%20is%20 high%20blood,at%20their%20maximally%20tolerated%20doses
8. Manaktala, R., Tafur-Soto, J. D., & White, C. J. (2020). Renal artery stenosis in the patient with hypertension: Prevalence, impact and management. Integrated Blood Press Control, 20(13), 71-82. https://doi.org/10.2147/IBPC.S248579
9. Mayo Clinic. (n.d.). Renal artery stenosis [Image]. Retrieved December 1, 2023, from https://www.mayoclinic.org/diseases-conditions/renal-artery-stenosis/symptoms-causes/syc-20352777
10. Nair, R., & Vaqar, S. (May 22, 2023). Renovascular hypertension. StatPearls Publishing. Retrieved November 30, 2023, from https://www.ncbi.nlm.nih.gov/books/NBK551587/
11. Nejad, S. H., Azzam, O., & Schlaich, M. P. (2023). Resistant hypertension: an approach to management. Medicine Today, 24(8), 23-28. https://medicinetoday.com.au/mt/supplements/feature-article/resistant-hypertension-approach-management
12. Rountas, C., Vlychou, M., Vassiou, K., Liakopoulos, V., Kapsalaki, E., Koukoulis, G., Fezoulidis, I. V., & Stefanidis, I. (2007). Imaging modalities for renal artery stenosis in suspected renovascular hypertension: prospective intraindividual comparison of color Doppler US, CT angiography, GD-enhanced MR angiography, and digital substraction angiography. Renal Failure, 29(3), 295–302. https://doi.org/10.1080/08860220601166305
13. Saljoughian, M. (August 18, 2015). The role of renal artery stenosis. U.S. Pharmacist. Retrieved November 30, 2023, from https://www.uspharmacist.com/article/the-role-of-renal-artery-stenosis
14. Vipparla, N., Kichloo, A., Albosta, M. S., Aljadah, M., Wani, F., & Lone, N. (2020). Resistant hypertension secondary to severe renal artery stenosis with negative duplex ultrasound: a brief review of different diagnostic modalities. Journal of Investigative Medicine High Impact Case Reports, 8. ttps://doi.org/10.1177/2324709620914793
15. Weber, B. R., & Dieter, R. S. (2014). Renal artery stenosis: epidemiology and treatment. International Journal of Nephrology and Renovascular Disease, 7. https://doi.org/10.2147/IJNRD.S40175
16. Yadav, A., Buxi, T. B. S., Reddy, S., Ghuman, S. S., Rawat, K. S., & Gupta, S. (2015). CT abdominal angiography. Current Medicine Research and Practice, 5(1), 37-49. https://doi.org/10.1016/j.cmrp.2014.11.008