
July 15, 2018, Dr Chee L Khoo
It’s always sad to lose a patient due to complications of a disease. It’s even harder if the patient is another doctor especially if the disease has well recognised complications. Many of you may have read about the sad story of Dr Rana, known to have cystic fibrosis, who died of complications resulting from an unrecognised bowel obstruction. It was reported on Sydney Morning Herald few weeks ago.
Prior to 1980, most patients with cystic fibrosis died during infancy. As a result of multidisciplinary management, including treatment with pancreatic enzymes, anti-pseudomonal antibiotics, and lung transplant in some patients, many of our patients with cystic fibrosis are now living beyond the age of 50 years.
Cystic fibrosis is an autosomal recessive genetic disease, with an incidence of around 1 in 2500 livebirths in white population. Mutations in the gene encoding the cystic fibrosis transmembrane conductance regulator (CFTR)1 result in a non-functional CFTR protein causing restricted transport of chloride ions across epithelial cells of the respiratory, hepatobiliary, gastrointestinal, and reproductive tracts, and the pancreas. Dehydration and viscous secretions lead to luminal damage and obstructions in the affected organs.2 Progressive respiratory complications are the major cause of the increased morbidity and mortality.
Because an increasing number of patients with cystic fibrosis are surviving into adulthood, the number of patients being diagnosed with gastrointestinal malignancies has increased. Back in 1991, Neglia et al did not find any increase in GI cancers in a small cohort of 712 patients with cystic fibrosis1. However, Sheldon et al reported that the incidence of malignant tumours were 4 times higher in patients with CF compared with the general population2. The cohort had only 412 patients. These small studies may be underpowered to answer our question of whether patients with CF have higher risks of specific GI cancers. A recent meta-analysis seeks answers to that question.
99925 patients in 6 cohort studies were identified for the meta-analysis. The primary outcome measure was the incidence of GI cancer in patients with CF reported as standardised incidence ratios (SIR). They also looked at incidence of GI cancers in subgroup of patients who had lung transplants. The average follow up was 6.9 years.
Overall, patients with CF were 8 times more likely to have GI cancers compared with the general population. Specifically, the risk of small bowel cancers were increased 18.94 times, colon cancer 10.91 times, biliary tract cancers 17.87 times and pancreatic cancer 6.18 times. The risks in patients who had transplants were 5 times higher than those that did not.
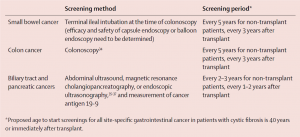
Wow, these are significantly higher risks of malignancies in patients with CF. The (US) Cystic Fibrosis Foundation Task Force now recommends colon cancer screening begin after 40 years with repeat screening every 5 years but every 3 years after transplant3. There are also recommendations for surveillance for small bowel, biliary tract and pancreatic cancers (see table 1).
Fortunately, many of our patients with CF are closely followed up at Westmead Hospital but they may present to us as family doctors in between those hospital visits. Awareness of their risks and high index of suspicions in these patients are warranted.
Access abstract here.
Reference
- Neglia JP, Wielinski CL, Warwick WJ. Cancer risk among patients with cystic fibrosis. J Pediatr 1991; 119: 764–
- Sheldon CD, Hodson ME, Carpenter LM, Swerdlow AJ. A cohort study of cystic fibrosis and malignancy. Br J Cancer 1993; 68: 1025–
- Hadjiliadis D, Khoruts A, Zauber AG, et al. Cystic Fibrosis Colorectal Cancer Screening Consensus Recommendations. Gastroenterology 2017; 154: 736–e16.
- Akihiro Yamada, Yuga Komaki, Fukiko Komaki, Dejan Micic, Samantha Zullow, Atsushi Sakuraba. Risk of gastrointestinal cancers in patients with cystic fibrosis: a systematic review and meta-analysis. Lancet Oncol 2018; 19: 758–67.