
14th January 2023, NIA Diagnostic Imaging
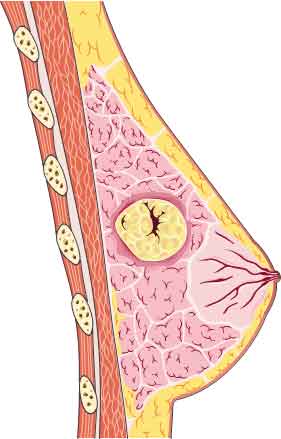
Despite the availability of modalities such as mammography, MRI and galactography, ultrasound still has a role in breast imaging. Ultrasound provides high resolution portrayal of normal and abnormal breast parenchyma as well as clear depiction of lactiferous ducts and the terminal duct-lobular unit where masses can form (4). This is particularly useful when investigating women presenting with a bloody nipple discharge.
Intraductal papillomas (IP) are benign tumours that emerge from the breast duct epithelium and are a frequent cause of bloody nipple discharge (6). Although benign, they are considered high-risk precursor lesions due to their association with ductal carcinoma in situ (DCIS), atypical ductal hyperplasia (ADH) and carcinoma.
Risk factors for developing breast tumours include: family history; radiation exposure; increasing age; hormone replacement therapy; and contraceptive use (3).
IPs can form in different areas of the mammary ducts and their location determines their type. Papillomas found in the subareolar region are distinguished as the ‘central’ type, and these are solitary and most prevalent in women undergoing perimenopause. The other type are ‘peripheral’ papillomas and they develop within the terminal duct-lobular unit as multiple tumours and are more common in young females (6). The disease can occur at any age for both males and females, but they are mostly found in females aged 35-55 years (5).
IPs are formed by the rapid production of ductal epithelium bounded by myoepithelial cells and a fibrovascular stroma, and develops into smooth, well-defined nodules (2). The cells that make up these tumours can undergo abnormal changes such as epithelial hyperplasia and can also proliferate atypically and sclerotise which can create symptoms of nipple pain and pathological nipple discharge (3).
When more than 5 papillomas are detected, it is called papillomatosis and 10% of these conditions are associated with malignancy (5). In addition, molecular studies have found that solitary papillomas, papillomatosis, DCIS and ADH possess mutations of chromosome 16p and 16q – which further explains IP’s link to malignant diseases (1). Therefore, it is critical for the patient to have these lesions further investigated via percutaneous core biopsies to confirm diagnosis and exclude presence of carcinoma.
NIA Diagnostic Imaging is equipped with state-of-the-art ultrasound machines to acquire high definition visualisation of breast tissue. This intervention can be conducted at any NIA Diagnostic Imaging sites (Glenquarie or Ingleburn) by experienced male and female radiologists, and are BULK-BILLABLE.
NIA Diagnostic Imaging is also equipped with the latest breast tomosynthesis (3D mammography) to further aid in breast cancer detection, and this is also BULK-BILLABLE for non-screening referrals.
References
- Agoumi, M., Giambattista, J. & Hayes, M., 2016. Practical Considerations in Breast Papillary Lesions: A Review of the Literature. Archives of Pathology & Laboratory Medicine, 140(8), pp. 770-290.
- Aljarrah, A. et al., 2015. Diagnostic dilemmas in Intraductal papillomas of the breast – Experience at Sultan Qaboos University Hospital in the Sultanate of Oman. Pakistan Journal of Medical Sciences, 31(2), pp. 431-434.
- Li, A. & Kirk, L., 2020. Intraductal Carcinoma, Treasure Island: StatPearls Publishing.
- Malherbe, K. & Annamaraju, P., 2021. Breast Ultrasound, Treasure Island: StatPearls Publishing.
- Nunez, D. L. et al., 2020. Papillary lesions of the breast: a review. Breast Cancer Management, 9(4).
- Tarallo, V., Canepari, C. & Bortolotto, C., 2012. Intraductal papilloma of the breast: A case report. Journal of Ultrasound, 15(2), pp. 99-101.