
A/Prof Chee L Khoo, 26th January 2025

Obesity was first recognised as a disease by WHO in 1948, and more recently also by several medical societies and countries (1–9). The current WHO International Classification of Disease labels obesity as “a chronic complex disease”. But obesity is a highly heterogenous condition and many people with excess adiposity have no signs of illness. One of the reasons for this is, perhaps, we are not diagnosing obesity correctly or accurately. We are used to using body mass index (BMI) to categorise different degrees of adiposity. However, using BMI to diagnose or exclude obesity can lead to a lot of overdiagnosis especially in muscular subjects or a lot of underdiagnosis especially in elderly subjects and in certain ethnic groups.
BMI was first invented by Belgian astronomer, mathematician, statistician, and sociologist, Adolphe Quetelet in the early 19th century as a means to see whether a person has a healthy weight compared with the general population. It was not intended to assess individual fatness or as a means of a medical assessment. BMI has been used to assess the degree of adiposity and of course, classes of obesity based on BMI have been created and often, management is based on these classes of obesity.
Another problem with managing obesity is the debate about whether obesity is a risk factor or is an actual disease in its own right. Further, the “co-morbid” medical conditions are sometimes considered to be caused by obesity and lumped together with the complications of obesity. There are not the same and their management differ. Treatment of obesity alone may not address the other associated metabolic conditions but may treat diseases which are complications of obesity.
The Lancet initiated a Commission to sort out the mess in the diagnosis and management of obesity (10). This is 4.5 years of monthly meeting amongst 58 experts in the field. The Commission is a 42-page document and I would like share the relevant gist of the document with you in this article.
The Lancet Commission’s New Diagnostic Model for Obesity
The Commission concluded “that a blanket definition of obesity as a disease would entail an unacceptably high risk of overdiagnosis”. The Commission summarised a number of clinical entities:
Obesity or excessive adiposity just define the phenotype and does not define a disease as not everyone who are obese have a disease. For example, not everyone who is obese is insulin resistant or has obstructed sleep apnoea.
Clinical obesity, is a systemic, chronic illness directly and specifically caused by excess adiposity. It provides a more coherent explanation of why obesity can fulfil the generally accepted criteria of a disease state in certain circumstances.
Pre-clinical obesity is the clinical state where there is excess adiposity but the function of all organs potentially affected by obesity is preserved. It is not limited to the lack of metabolic dysfunction as we know obesity can lead to mechanical, respiratory dysfunction and other activity of daily living dysfunctions (see below). Preclinical obesity is not the same as metabolically healthy obese.
Pre-clinical obesity is also different from pre-obesity. Pre-obesity is a subset of patients with increasing levels of excessive adiposity which is not considered obese yet whereas patients with pre-clinical obesity has confirmed obesity (see below).
Confirmation of the Obesity Phenotype
While BMI is not the end all in the diagnosis of obesity, it is still a good starting point. Patients in front of us who look like they may have excess adiposity or has a high BMI probably are obese but we need to confirm the diagnosis of obesity with at least one other anthropometric measurement – waist, waist-hip or waist height measurements or via a dual-energy-xray-absorptiometry (DEXA) scan. See Figure 1 for anthropometric cut-offs.

Once the anthropometric measures confirm that the patient has excess adiposity, the patient has obesity. They may or may not have clinical disease, though. So we need to take a history and examination of the patient and likely, organise further investigations to look for the presence of organ dysfunction.
Measurements of waist circumference and waist-to-hip ratio can vary across populations and between sexes. These measurements might not accurately reflect subcutaneous and visceral fat accumulation. Although using anthropometric measures as alternatives or in addition to BMI could improve detection of excess adiposity and prediction of cardiometabolic risk, akin to BMI they are not a robust measure of ongoing illness.
See Figure 2 for the steps in diagnosing clinical obesity.
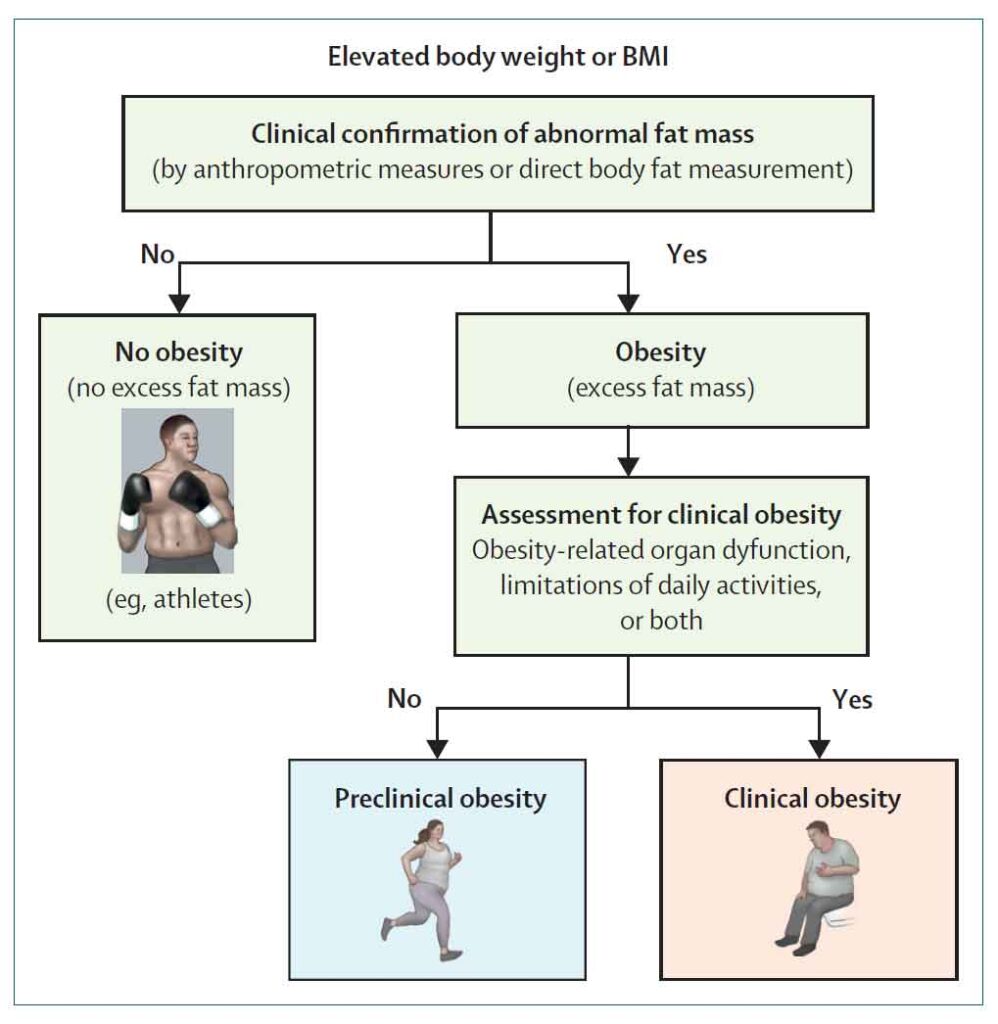
Looking for Clinical Obesity
Once we have the presence of obesity confirmed by additional anthropometric measures, we need to look for the presence (or absence) of organ or functional dysfunction. This is not just the traditional metabolic dysfunction of dysglycaemia, hypertriglyceridaemia, fatty liver disease, heart failure etc but include physical limitations of daily living related to musculoskeletal dysfunction, respiratory limitations or airway obstructions (peripheral or central sleep apnoea) due for the excessive adiposity. It also include skin conditions, genito-urinary abnormalities and reproductive deficiencies in both male and females. See Figure 3 for the full listing of the associated conditions.
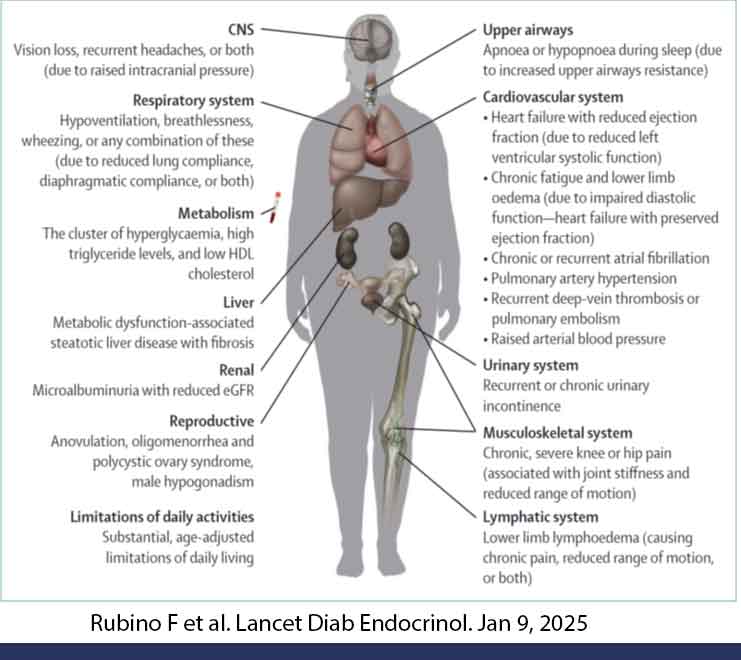
From here, we can then decide whether this patient have just an obese phenotype and no organ dysfunction (pre-clinical obesity) or obese phenotype plus a chronic illness as described above (clinical obesity).
Why is this new definition important?
It does matter in the management whether the obese patient has clinical obesity or preclinical obesity. There are many causes of obesity. Not everyone with obesity will have obesity related illnesses. This Commission reminds us to look for the other medical conditions as the management of clinical obesity must include management of associated medical conditions as well as the complications of obesity. We need to individualise our approach to the patient in front of us. We are aiming for health goals and not weight goals. Yes, we need to work with the patient as they will be aiming for weight goals.
References:
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004; 363: 157–63.
- WHO. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. WHO technical report series 894. World Health Organisation, 2000.
- Carruba MO, Busetto L, Bryant S, et al. The European Association for the Study of Obesity (EASO) endorses the Milan Charter on Urban Obesity. Obes Facts 2021; 14: 163–68.
- American Society for Metabolic and Bariatric
Surgery. Consensus statement on obesity as a disease.
Consensus Statement on Obesity as a Disease
(accessed Dec 6, 2023). - Bray GA, Kim KK, Wilding JPH. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev 2017; 18: 715–23.
- Rathbone JA, Cruwys T, Jetten J, Banas K, Smyth L, Murray K. How conceptualizing obesity as a disease affects beliefs about weight, and associated weight stigma and clinical decision-making in health care. Br J Health Psychol 2023; 28: 291–305.
- Kim B-Y, Kang SM, Kang J-H, et al. 2020 Korean Society for the Study of Obesity guidelines for the management of obesity in Korea. J Obes Metab Syndr 2021; 30: 81–92.
- Mechanick JI, Garber AJ, Handelsman Y, et al. American Association of Clinical Endocrinologists’ position statement on obesity and obesity medicine. Endocr Pract 2012; 18: 642–48.
- Eisenberg D, Shikora SA, Aarts E, et al. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) indications for metabolic and bariatric surgery. Obes Surg 2023; 33: 3–14.
- Definition and diagnostic criteria of clinical obesity Rubino, Francesco et al. The Lancet Diabetes & Endocrinology, Volume 0, Issue 0