
14th May 2025, NIA Diagnostic Imaging
Coronary artery calcium (CAC) scoring is a well-established, non-invasive imaging technique for assessing cardiovascular risk by identifying and quantifying calcified plaque in the coronary arteries. The CAC score, a direct marker of subclinical atherosclerosis, highly predicts future cardiovascular events, making it an essential tool for clinicians in assessing risk, even in asymptomatic individuals. (4, 5)
CAC scoring facilitates early identification of at-risk individuals by providing an objective assessment of coronary artery disease (CAD) burden, allowing for more targeted and proactive cardiovascular health care. (5).
INTERPRETING CORONARY ARTERY CALCIUM SCORE RESULTS
Through the evaluation of calcified plaque, CAC scoring delivers essential insights regarding cardiovascular risk, even in asymptomatic individuals. The score helps clinicians gauge the extent of atherosclerotic burden, guiding treatment and risk management strategies. (4).
A higher CAC score generally indicates a greater likelihood of future cardiovascular events, prompting aggressive intervention methods. Conversely, a low or zero score indicates a minimal risk of heart disease, potentially reducing the need for immediate treatment. (5).
The CAC score can be interpreted as follows:
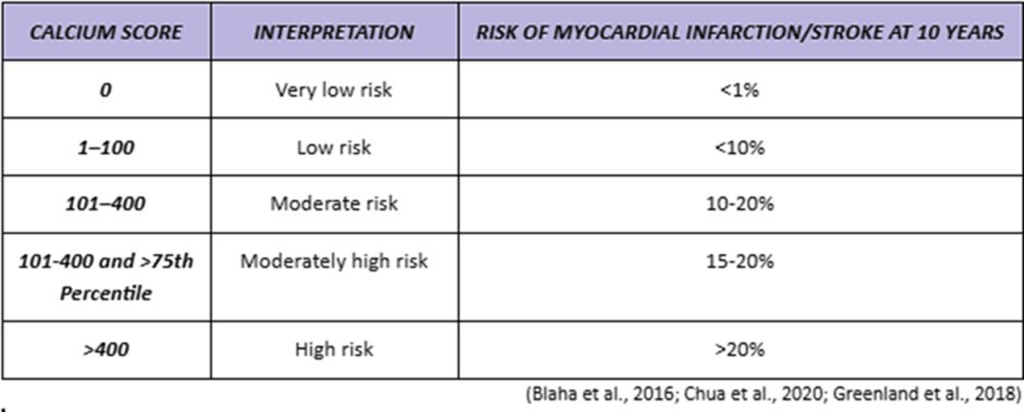
Nonetheless, as with any diagnostic test, the CAC score is only one component of the overall risk assessment and should be utilised in conjunction with other clinical factors, including patient history, lifestyle, and other biomarkers to provide a more comprehensive evaluation of cardiovascular risk.
WHEN TO REFER FOR CALCIUM SCORE
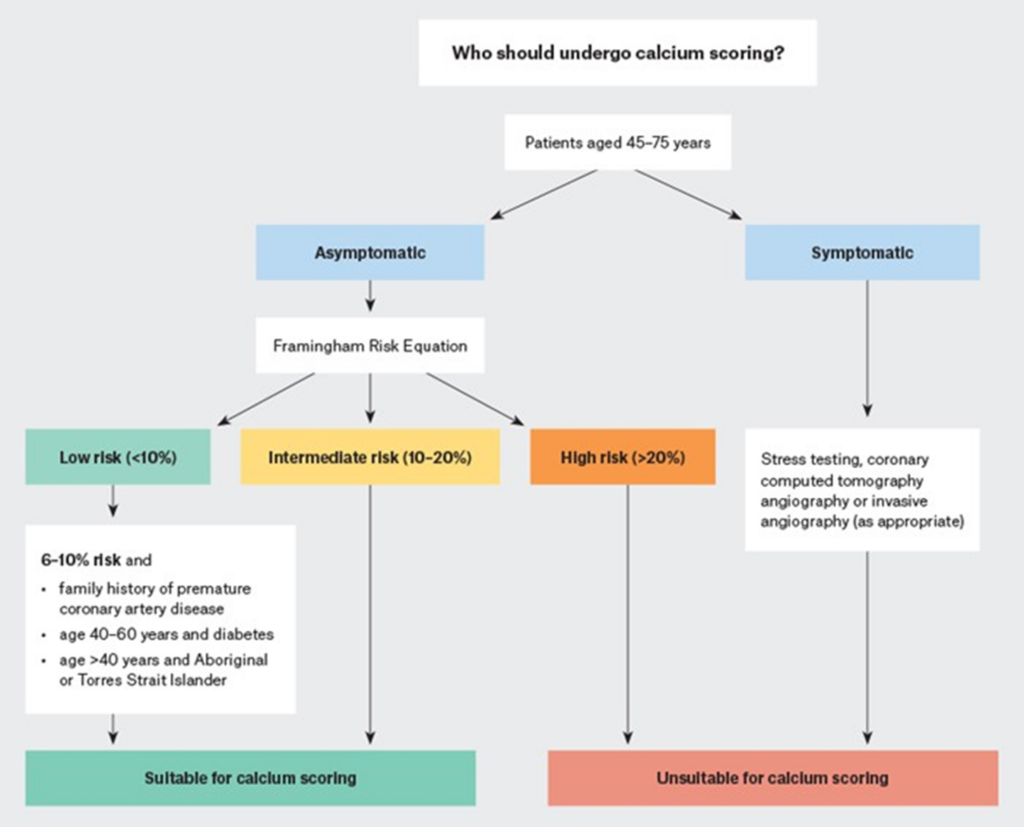
To assess which individuals are suitable for a CAC score, the Cardiac Society of Australia and New Zealand (CSANZ) recommends using the Framingham Risk Score. Following an initial evaluation using the Framingham risk score, the CSANZ recommends calcium scoring for asymptomatic persons at intermediate Framingham risk. Moreover, CAC scoring may also be effective for lower-risk patients (6-10% 10-year risk) who have concerning traits that the Framingham Risk Equation does not account for. This group includes Aboriginal and Torres Strait Islander individuals, as well as individuals with a strong family history of early CAD or diabetes. (2)
CAC scores are not beneficial for high-risk or very low-risk patients (≤6% 10-year risk), as they have limited ability to reclassify cardiovascular risk. Additionally, CSANZ does not recommend using calcium scoring for symptomatic patients as there is inadequate evidence to support its use over functional exams such as CT angiography and invasive coronary angiography. (2)
The following image outlines the recommended indications for CAC scoring, as provided by the CSANZ.
CONCLUSION
CAC scoring is a valuable tool for refining cardiovascular risk assessment, especially in asymptomatic individuals at intermediate risk. It supports early intervention and personalised prevention strategies. When used in conjunction with clinical judgment and established guidelines, such as those from the CSANZ, CAC scoring enhances decision-making and contributes meaningfully to preventive cardiology.
At NIA Imaging, we provide advanced coronary artery calcium (CAC) scoring to accurately evaluate your risk
of heart disease. Using cutting-edge technology and a skilled team, we deliver fast, non-invasive scans that support informed treatment and prevention decisions.
REFERENCES
Blaha, M. J., Mortensen, M. B., Kianoush, S., Tota-Maharaj, R., & Cainzos-Achirica, M. (2017). Coronary Artery Calcium Scoring. JACC: Cardiovascular Imaging, 10(8), 923–937. https://doi.org/10.1016/j.jcmg.2017.05.007
Chua, A., Blankstein, R., & Ko, B. (2020). Coronary artery calcium in primary prevention. Australian Journal of General Practice, 49(8), 464–
469. https://doi.org/10.31128/ajgp-03-20-5277
Gami, A., Bisht, S., Satish, P., Blaha, M. J., & Patel, J. (2024). The utility of coronary artery calcium scoring to enhance cardiovascular risk assessment for South Asian adults. Progress in cardiovascular diseases, 84, 7–13. https://doi.org/10.1016/j.pcad.2024.05.001
Goff, D. C., et al. (2021). Coronary artery calcium score and cardiovascular risk prediction: Current insights. Journal of the American College of Cardiology, 78(9), 915-925. https://doi.org/10.1016/j.jacc.2021.07.043
Greenland, P., Blaha, M. J., Budoff, M. J., Erbel, R., & Watson, K. E. (2018). Coronary calcium score and cardiovascular risk. Journal of the American College of Cardiology, 72(4), 434–447. https://doi.org/10.1016/j.jacc.2018.05.027
Hecht, H., Blaha, M. J., Berman, D. S., Nasir, K., Budoff, M., Leipsic, J., Blankstein, R., Narula, J., Rumberger, J., & Shaw, L. J. (2017). Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography. Journal of cardiovascular computed tomography, 11(2), 157–168. https://doi.org/10.1016/j.jcct.2017.02.010
Khan, S. S., Post, W. S., Guo, X., Tan, J., Zhu, F., Bos, D., Sedaghati-Khayat, B., van Rooij, J., Aday, A., Allen, N. B., Bos, M. M., Uitterlinden, A. G., Budoff, M. J., Lloyd-Jones, D. M., Mosley, J. D., Rotter, J. I., Greenland, P., & Kavousi, M. (2023). Coronary Artery Calcium Score and Polygenic Risk Score for the Prediction of Coronary Heart Disease Events. JAMA, 329(20), 1768–1777. https://doi.org/10.1001/jama.2023.7575
Limpijankit, T., Jongjirasiri, S., Meemook, K., Unwanatham, N., Thakkinstian, A., & Laothamatas, J. (2023). Predictive values of coronary artery calcium and arterial stiffness for long-term cardiovascular events in patients with stable coronary artery disease. Clinical cardiology, 46(2), 171–183. https://doi.org/10.1002/clc.23955
Neves, P. O., Andrade, J., & Monção, H. (2017). Coronary artery calcium score: current status. Radiologia brasileira, 50(3), 182–189. https://doi.org/10.1590/0100-3984.2015.0235