
9th November 2024, NIA Diagnostic Imaging
What is shoulder bursitis?
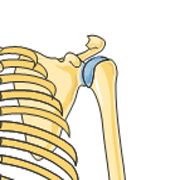
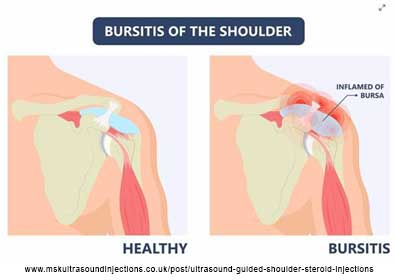
Shoulder bursitis is one of the most common causes of shoulder pain and is referred as an inflammatory disorder affecting the subacromial-subdeltoid bursa (Faruqi & Rizvi, 2023). The subacromial-subdeltoid bursa is a fluid-filled sac lined with synovium which separates the supraspinatus tendon from the acromion, coracoacromial ligament and deltoid and helps ease movement between the rotator cuff and other structures of the shoulder joint (MacMahon & Yablon, 2017).
What are the causes of shoulder bursitis?
Shoulder bursitis often results from repetitive overhead activities that place strain on the shoulder, leading to impingement as well as by minor injuries such as falls (Faruqi & Rizvi, 2023). However, the underlying causes of shoulder bursitis are often complex and multifactorial, involving factors such as altered biomechanics, age-related degeneration, and in some cases, systemic inflammatory conditions (Lo et al., 2022). While overuse is a predominant contributor, other factors like poor posture, previous shoulder injuries, or even genetic predispositions may also play a role in its development (Lo et al., 2022).
Ultrasound imaging for shoulder bursitis
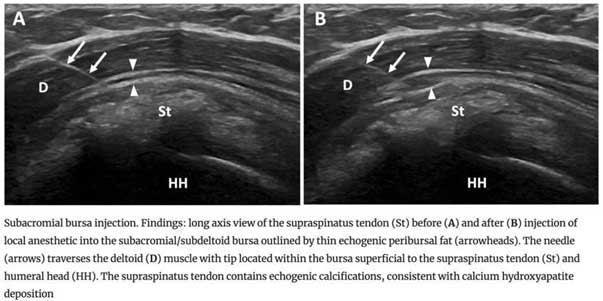
The subacromial-subdeltoid bursa is normally seen sonographically as a thin (2mm in thickness), anechoic fluid-filled structure with a hyperechoic peribursal fat border (MacMahon & Yablon, 2017). If there is increased fluid (hypoechoic or complex appearance), thickening of the bursal walls, or a change in the normal structure, this suggests bursitis or other shoulder pathologies. Bursal impingement is assessed with dynamic scanning of the patient’s shoulder during abduction and adduction (MacMahon & Yablon, 2017). Free gliding movement of the supraspinatus beneath the acromion should be demonstrated (Jacobson, 2018). Signs of bursal impingement can include pain on abduction, bunching and pooling of bursal fluid and pain (Jacobson, 2018).
Treatment
Treatment for shoulder bursitis aims to reduce inflammation, relieve pain, and restore normal function of the shoulder (Fawcett et al., 2018). The approach typically depends on the severity of the condition and whether it is associated with other shoulder problems, such as rotator cuff tendinopathy or impingement syndrome (Fawcett et al., 2018).
Corticosteroid injections are often recommended as an effective non-surgical treatment to alleviate symptoms of bursitis (Hseih et al., 2023). During the injection, a fine needle is carefully inserted into the affected bursa under ultrasound guidance. Once in position, a combination of local anaesthetic and cortisone is injected directly into the area, which helps to reduce inflammation and swelling over time and potentially provide longer-term pain relief (Hseih et al., 2023).
This method enhances the accuracy of the injection, reduces the risk of complications, and minimises discomfort for the patient by ensuring that the medication is delivered precisely to the site of inflammation (McGill et al., 2022). By targeting the source of the pain with precision, ultrasound-guided corticosteroid injections can significantly improve outcomes for individuals with bursitis, helping them regain mobility and function more quickly (McGill et al., 2022).
NIA Diagnostic Imaging performs these injections on a regular basis and has helped hundreds of patients to regain their mobility and return back to normal every day activities. Furthermore, NIA Diagnostic Imaging bulk-bills all musculoskeletal ultrasound as well as all cortisone injections.
References
Faruqi, T. & Rizvi, T. J. (2023). Subacromial bursitis. StatPearls Publishing. Retrieved 20th October 2023, from https://www.ncbi.nlm.nih.gov/books/NBK541096/#:~:text=Subacromial%20bursitis%20is%20an%20inflammatory,the%20etiology%20can%20be%20multifactorial
Fawcett, R., Grainger, A., Robinson, P., Jafari, M., & Rowbotham. (2018). Ultrasound-guided subacromial-subdeltoid bursa corticosteroid injections: A study of short- and long-term outcomes. Clinical Radiology, 73(8). doi:10.1016/j.crad.2018.03.016
Hseih, L.-F., Kuo, Y.-C., Hunag, Y.-H., Liu, Y.-F., & Hsieh, T.-L. (2023). Comparison of corticosteroid injection, physiotherapy and combine treatment for patients with chronic subacromial bursitis-A randomised controlled trial. Clinical Rehabilitation, 37(9). doi: 10.1177/02692155231166220
Jacobson, J. A. (2018). Fundamentals of musculoskeletal ultrasound. (3rd ed.). Elsevier
Lo, C. N., van Griensven, H., & Lewis, J. (2022). Rotator cuff related shoulder pain: An update of potential pathoaetiological factors. New Zealand Journal of Physiotherapy, 50(2), 82-93. doi:10.15619/NZJP/50.2.05
McGill, K. C., Patel, R., Chen, D., & Okwelogu, N. (2023). Ultrasound-guided bursal injections. Skeletal Radiology, 52, 967-978. doi: 10.1007/s00256-022-04153-y
McMahon, C. & Yablon, C. (2017). The Shoulder. In C. M. Rumack & D. Levine (Eds.), Diagnostic ultrasound (5th ed., pp. 877-897). Elsevier.