
13th February 2026, NIA Diagnostic Imaging

Trigger finger is a common hand condition that often presents in primary care. It often starts as more an annoyance to the patient but eventually, as it deteriorates, affects the normal functioning of the hand. The only management option used to be surgical release of the tendon. We now have another management option – ultrasound guided cortisone injection.
Trigger finger is a condition that causes pain, stiffness, clicking, or locking of a finger or thumb. Symptoms often occur when bending or straightening the finger and are usually worse in the morning. Trigger finger develops when the flexor tendon or the A1 pulley becomes thickened or inflamed, preventing the tendon from gliding smoothly during movement (Makkouk et al., 2021).
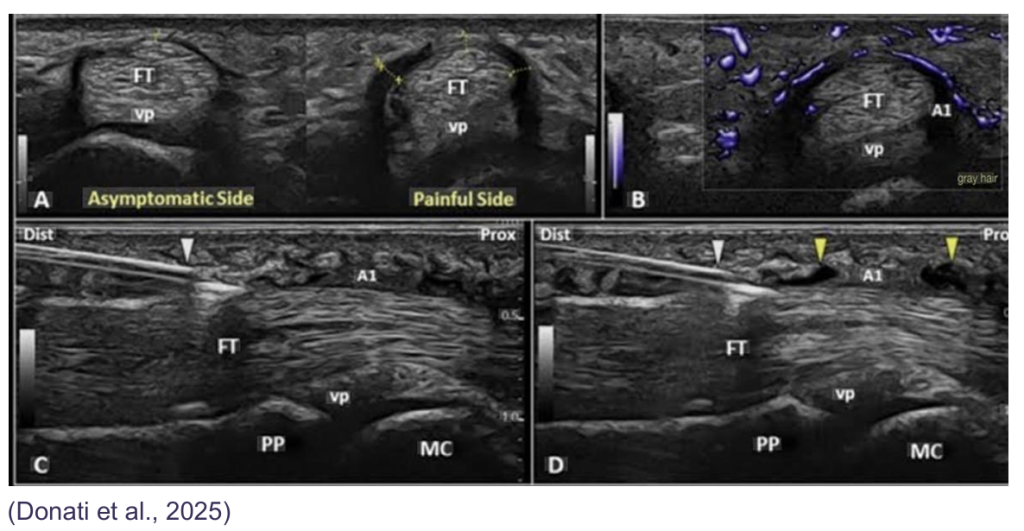
Trigger finger is often diagnosed clinically, but ultrasound is useful in confirming the diagnosis and assessing severity, especially when symptoms persist or the presentation is unclear. Ultrasound commonly shows thickening of the A1 pulley, swelling of the flexor tendon, fluid around the tendon sheath, and visible tendon catching during finger movement (Draghi & Bortolotto, 2020; Lee et al., 2022). Dynamic ultrasound allows the tendon to be assessed in real time as the finger moves.
Corticosteroid (cortisone) injection is a well-established and effective treatment for mild to moderate trigger finger. Cortisone reduces inflammation within the tendon sheath, allowing smoother tendon movement. Ultrasound-guided injections improve accuracy and reduce the risk of complications compared with landmark-guided injections (Ryzewicz & Wolf, 2021; Wu et al., 2023).
Most patients improve within days to weeks after injection. If symptoms persist or recur, a repeat injection or surgical release of the A1 pulley may be considered. Surgery is generally reserved for cases that do not respond to conservative treatment and has a high success rate (AAOS, 2024).
Conclusion: Ultrasound is a valuable tool in the assessment and management of trigger finger. It helps confirm the diagnosis, evaluate severity, and guide cortisone injection, supporting effective and targeted patient care

References:
References References American Academy of Orthopaedic Surgeons. (2024). Trigger finger (stenosing tenosynovitis): Clinical practice guidance. AAOS. Donati, D., Ricci, V., Boccolari, P., Tedeschi, R., Origlio, F., Vita, F., Naňka, O., Catani, F., & Tarallo, L. (2025). Trigger Finger: A narrative review of dynamic ultrasound and personalized therapies. Journal of Clinical Ultrasound, 53(5), 1111–1121. https://doi.org/10.1002/jcu.23971 Draghi, F., & Bortolotto, C. (2020). Ultrasound evaluation of trigger finger. Journal of Ultrasound, 23(2), 123–130. https://doi.org/10.1007/s40477-020-00450 7 Lee, D. H., Lee, S. H., & Gong, H. S. (2022). Role of ultrasound in the diagnosis and management of trigger finger. Ultrasonography, 41(1), 23–30. https://doi.org/10.14366/usg.21060 Makkouk, A. H., Oetgen, M. E., Swigart, C. R., & Dodds, S. D. (2021). Trigger finger: Etiology, evaluation, and treatment. Journal of the American Academy of Orthopaedic Surgeons, 29(10), 444–452. https://doi.org/10.5435/JAAOS-D-20-00965 Ryzewicz, M., & Wolf, J. M. (2021). Corticosteroid injection for trigger finger: Indications and outcomes. Hand Clinics, 37(2), 145–151. https://doi.org/10.1016/j.hcl.2021.01.004 Wu, Y. T., Ke, M. J., & Chou, Y. C. (2023). Ultrasound-guided versus landmark-guided corticosteroid injection for trigger finger: A comparative study. Skeletal Radiology, 52(5), 987–994. https://doi.org/10.1007/s00256-023-04155-9