
1st September, 2018, Dr Chee L Khoo
It would seem to me that just about every doctor who graduated from Australian medical schools know about Morton’s neuroma. It’s part of the long list of differential diagnoses of forefoot pain but either I have missed many or it’s not that common. I’m also not sure what else to do once diagnosed apart from referring to an orthopaedic surgeon. Surely, there must be other modalities of treatment apart from surgery. Further, is it really a neuroma? And have you ever wonder why it’s always in the third web space?
The condition was first described by Civinini in 1835 as a fusiform swelling of the common digital nerve of the third web space. Queen Victoria’s chiropodist published a discussion paper on the condition later but the condition was named after Thomas Morton, an American orthopaedic surgeon who published his case series of 15 patients with the condition in 1876. He attributed the neuralgia to injury to the fourth metatarsophalangeal joint. It’s actually not a neuroma at all. Histological studies showed that it is a proliferative fibrosis of the peri-neural tissue.
So why does it occur only in the third web space? To answer that question, we need to examine the anatomy of the foot and its innervation of the plantar skin. The skin of the plantar su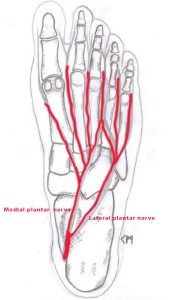 rface of the foot is innervated by the medial and lateral plantar nerves which are branches of the tibial nerve. The medial plantar nerves supplies the skin of the medial three and a half toes while the lateral plantar nerves supplies the lateral one and half toes. Significantly, the digital nerve to the third web space receives a major branch from the lateral plantar nerve (see figure 1). The common digital nerve passes deep to the deep transverse metatarsal ligament (DTML) which is the ligament that holds the metatarsal head together.
rface of the foot is innervated by the medial and lateral plantar nerves which are branches of the tibial nerve. The medial plantar nerves supplies the skin of the medial three and a half toes while the lateral plantar nerves supplies the lateral one and half toes. Significantly, the digital nerve to the third web space receives a major branch from the lateral plantar nerve (see figure 1). The common digital nerve passes deep to the deep transverse metatarsal ligament (DTML) which is the ligament that holds the metatarsal head together.
There are numerous theories on the aetiology of the “neuroma”. They include repetitive traction injury from dorsiflexion of the toes, inflammatory bursitis of the intermetatarsal joints causing fibrosis in the webspace, entrapment of the common digital nerve at the anterior edge of the DTML and ischaemia from the degenerative changes in the plantar arteries. They remain theories but the aetiology must have something to do with the biomechanics of the forefoot articulation. It is more common with patients wearing narrow shoes and high heels. Symptoms are relieved by footwear change and massaging.
Diagnosis
It is tempting for doctors to image everything we see to “confirm” the diagnosis. Plain xrays are essential to exclude stress fractures, avascular necrosis of the second metatarsal or osteoarthritis of the metatarsophalangeal joint. The MRI recently showed a sensitivity 93% with specificity 68%, while the ultrasound sensitivity was 90% and specificity 88% but the finding of an enlargement of the digital nerve can be an incidental finding. The diagnosis of Morton’s neuroma is a clinical one. Squeezing the heads of the metatarsals with one hand and putting pressure in the third webspace with the other hand will induce the pain.
Conservative treatment
Modification of footwear have been shown to improve symptoms in up to 41% of patients. Plantar orthosis for metatarsal offloading has been reported with some success.
Steroid injection provides long term relief only in a small proportion of patients. Amongst those that responded, 95% remained asymptomatic after two years. However, repeated steroid injection can lead to plantar fat atrophy or rupture of the metatarsophalangeal joint capsule. Other forms of injections tried include botox and alcohol. Radiofrequency nerve ablation has also been tried. Long term results are either lacking or poor.
Surgical treatment
The traditional approach is open neurectomy – the excision of the neuroma as proximal as possible. Success rate ranges from 51 – 85%. Surgeons who believe in the entrapment theory perform decompression by releasing the DTML. They claim success rates of 95%. Most surgeons use the dorsal approach which avoid scars in the weight bearing plantar surface. The plantar approach provides better visualisation and obviates the need to cut the DTML.
I guess, like everything else in orthopaedics, we need to look for the cause of the metatarsalgia. Is it to do with repetitive trauma to the metatarsal joints? Is it to do with faulty footwear? A period of conservative measures including a trial of cortisone injection may be worthwhile. Perhaps, a referral to a podiatrist who has special interest in bio-mechanics may be helpful.
Reference
Sameer Jain, Ken Mannan. The Diagnosis and Management of Morton’s Neuroma. A Literature Review. Foot and Ankle Specialist Aug 2018, 6 (4); 307-317
Francesco Di Caprio, Renato Meringolo, Marwan Shehab Eddine, Lorenzo Ponziani. Morton’s interdigital neuroma of the foot A literature review. Foot and Ankle Surgery 24 (2018) 92–98