
22nd April 2019, Dr Chee L Khoo
One of the diagnoses I dread to miss in general practice is slipped capital femoral epiphysis (SCFE). It is not common (yet) but most general practitioners will encounter (or miss) a few of these in their life time. They are mostly seen during the adolescent years and are more prevalent although not exclusively, in the overweight and obese. Pain is the most common symptom but the site of pain can vary. There are “typical” and “atypical” pain patterns. Recognising both the “typical” and “atypical” pain patterns may assist us in making an earlier diagnosis and reduce complications of worsening deformity, avascular necrosis and osteoarthritis.
Pain associated with osteoarthritis is well described in adults but less so in children. Pain described is generally present in the groin, hip, thigh, or knee. If the diagnosis is delayed, anterolateral and superior displacement of the metaphysis relative to the epiphysis progresses. Aspects of the history which can suggest SCFE include an inciting event, recent growth spurt, pain with exercise or stairs, or a predisposing medical history such as obesity or other endocrine disease.
External rotation of hip and an out-toeing gait become apparent. Limited internal rotation with the hip flexed to 90 degrees is characteristic at this stage of deformity. Hip abduction, flexion, and internal rotation are reduced. There is often obligate external rotation with hip flexion. Pain may be elicited with resisted straight leg raise. Patients often demonstrate a limp.
So, what is “typical pain” in SCFE? In a prospective study involving 110 adolescents between 8 and 16 years old diagnosed with SCFE and admitted to a tertiary children’s hospital for surgery, researchers attempted to identify the patterns of pain in SCFE.
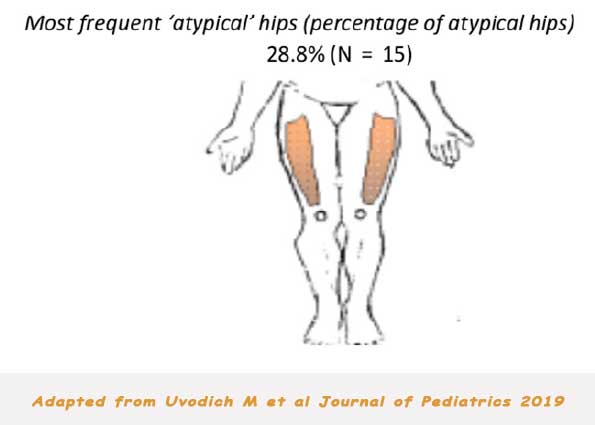
The children in the study completed a standard pain diagram localising the site of pain. Typical pain was defined as presence of anterior hip pain and atypical pain was pain that did not include the anterior hip. Combination pain was defined as pain in more than one location. Stable SCFE was defined as being able to ambulate with or without crutches, and unstable SCFE was defined as the in ability to bear weight at all. The number of health practitioner visits before a diagnosis was noted.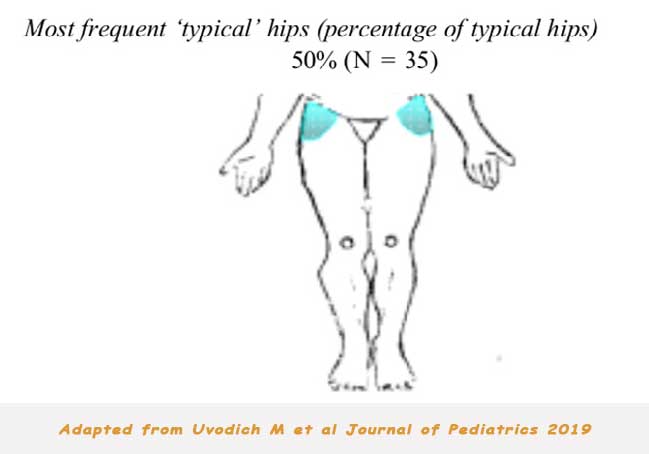
The mean age of the patient population was 12.2 years, 61% were male, and the mean weight percentile for age was 89.3. Sixty-seven patients had 1 pain zone designated, most commonly the hip, thigh, and knee. Combination pain was present in 48 (39%) of the 122 hips.
As expected, hip pain was the most common location among affected hips. Posterolateral thigh pain was almost always seen (7 of 8 times). 36 of the 46 hips with combination pain had pain present in the hip. The 2 most common non-hip combinations were groin/thigh (n = 4) and thigh/knee (n = 3). There were 2 patients with pain located below the knees, 1 with pain in the shin, and 1 with pain in the ankles.
Hips with knee pain had a greater mean slip angle than those without. Those with combination pain had greater mean slip angles than those with an isolated pain location. An inciting incident was more associated with an unstable SCFE than not (P = .002). Those with an unstable slip were more likely to have hip pain than not compared with those with stable slip. Also, those with an unstable slip were more likely to have knee pain than those with a stable.
Radiographic interpretation is essential to the diagnosis of SCFE. Early radiographic findings include blurring and widening of the physis. Most of us no difficulty seeing a late slip but the trick is to pick an early slip. This is where a trusted radiology provider becomes vital.
The median duration of symptoms was 4 weeks. Duration of pain symptoms greater than 4 weeks was considered a delay in diagnosis for analysis. Another way of measuring delay in diagnosis is whether SCFE is diagnosed on the first symptomatic visit or not. They found that 49% of initial visits did not get the correct diagnosis made.
In an adolescent presenting with lower extremity pain, a diagnosis of SCFE should be considered. Clinical examination and confirmatory anterior/posterior pelvic and lateral radiographs should be considered. With increasing obesity among our children, the prevalence of SCFE will increase.
Access the abstract here.
Reference:
Uvodich M, Schwend R, Stevanovic O, Wurster W, Leamon J, Hermanson A. Patterns of Pain in Adolescents with Slipped Capital Femoral Epiphysis. Journal of Pediatrics. Volume 206, March 2019, Pages 184-189.