
25th December 2019, Dr Chee L Khoo
They used to call it “Paediatric Infection Triggered Autoimmune Neuropsychiatric Disorders” (PITANDS)(1). Sounds terrible, doesn’t it? They were referring to children with obsessive-compulsive disorder (OCD) who had a sudden onset of their psychiatric symptoms, typically following infection with a variety of agents, including group A streptococcus (pyogenes), varicella and mycoplasma pneumoniae. The subgroup specifically associated with group A streptococcus (GAS) was called “Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections” (PANDAS). Now that is beginning to sound better. There is more to come, though.
PANDAS was first described in 1998 in a clinically homogeneous cohort of children with OCD or tic disorders (2). Clinical assessments of more than 125 children and adolescents with OCD identified a unique subgroup of patients with unusually abrupt and dramatic OCD symptom onset and the presence of multiple neuropsychiatric comorbidities. The acute onset of OCD was fairly similar to the prodromal period of sydenham chorea (SC) and it was thought that this syndrome was an atypical form of SC.
The five diagnostic criteria in PANDAS consisted of OCD, prepubertal onset, abrupt onset, temporal association between symptom onset and GAS infection and associated neurological abnormalities (including choreiform movements). They required demonstration of a rise in ASO and anti-DNAaseB antbody titres to exclude cases not related to GAS infections.
The main criticisms of PANDAS were the difficulty in establishing a tight link between the inciting streptococcal infection and the onset/recrudescence of OCD or tic symptoms, and the lack of reliable biological markers. This led to a new clinical definition as proposed by Swedo et al in 2003, Pediatric Acute-Onset Neuropsychiatric Syndrome (PANS)(3). Of note, is the inclusion of anorexia as a primary criterion with or without OCD and the removal of the association with GAS infections.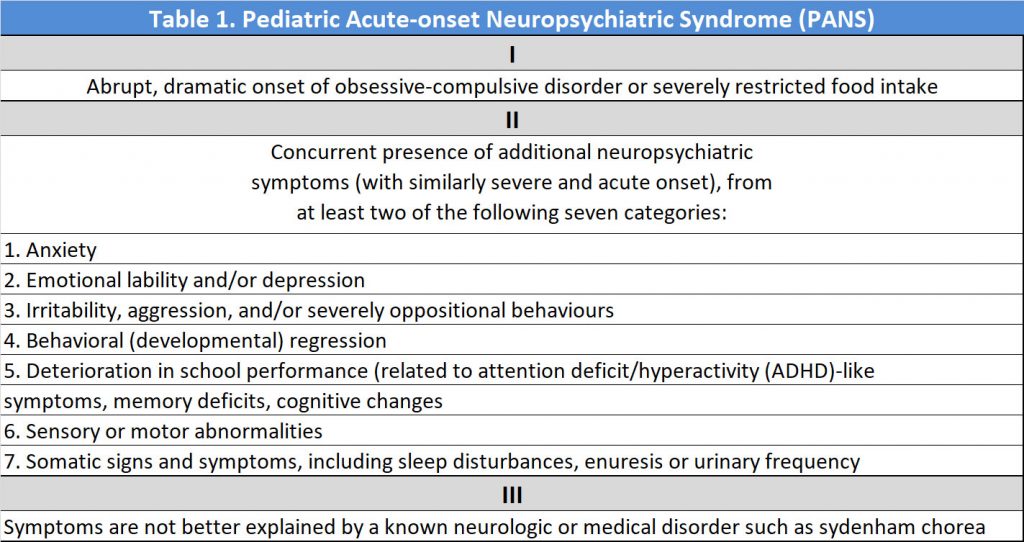
A second group of experts expanded the definition further by proposing the Childhood Acute Neuropsychiatric Syndrome (CANS) which increase the eligible age to under 18 years old and remove the association with any infection altogether (4).
When CANS/PANS is suspected, it is important to obtain a comprehensive medical and psychiatric history and perform a thorough physical examination. In particular, the family history should include review of neurologic diseases, psychiatric disorders, autoimmune and autoinflammatory diseases, immune-deficiency syndromes, and frequent infections, including recurrent streptococcal pharyngitis. First-degree relatives of children with PANDAS were noted to have increased rates of OCD, tic disorders, and acute rheumatic fever, suggesting that children may have inherited a specific vulnerability to nonpyogenic poststreptococcal sequelae (5). Neuropsychiatric disorders among siblings are particularly common and important to assess for as well. Psychiatric family history may provide important clues to genetic susceptibilities to OCD, anxiety, or mood disorders, ADHD, pervasive developmental disorder (PDD), and others.
As part of the diagnostic work up, all patients suspected of suffering from CANS/PANS should have:
- FBC, ESR, CRP
- Comprehensive metabolic panel
- Urinalysis (to assess hydration) and to rule out inflammation
- for children with urinary complaints; clean-catch urine culture
- for those with pyuria
- Throat culture, anti-streptolysin O (ASO) and anti-DNAse B
Further investigations may be necessary depending on the results of the preliminary screen.
Following diagnosis, the general principles of treatment involve:
- Psychotherapeutic treatment
- Antibiotic treatment
- Immuno-modulatory treatment
Because the CANS/PANS criteria define a broad spectrum of neuropsychiatric conditions, the syndrome is presumed to result from a variety of disease mechanisms and to have multiple aetiologies, ranging from postinfectious autoimmune and neuroinflammatory disorders to toxic, endocrine or metabolic disorders. The CANS/PANS entity still of unclear validity and not universal accepted. The evidence base for treatment with immunotherapy and/or psychological therapies for PANS is not strong.
There is a great need for better characterisation and long-term follow-up of this patient group to identify clinical and biological markers to guide treatment development. This is an evolving syndrome.
References:
- Allen AJ, Leonard HL, Swedo SE: Case study: A new infection triggered, autoimmune subtype of pediatric OCD and Tourette’s syndrome. J Am Acad Child Adolesc Psychiatry 34:307–311, 1995.
- Swedo SE, Leonard HL, Garvey M, Mittleman B, Allen AJ, Perlmutter S, Lougee L, Dow S, Zamkoff J, Dubbert BK: Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections:Clinical description of the first 50 cases. Am J Psychiatry 155:264–271, 1998. Erratum in Am J Psychiatry 155:578, 1998.
- Swedo SE, Leckman JF, Rose NR: From research subgroup to clinical syndrome: Modifying the PANDAS criteria to describe PANS (pediatric acute-onset neuropsychiatric syndrome). Pediatr Therapeut 2:1–8, 2012.
- Singer HS, Gilbert DL, Wolf DS, Mink JW, Kurlan R. Moving from PANDAS to CANS [published correction appears in J Pediatr. 2012 May;160(5):888]. J Pediatr. 2012;160(5):725–731. doi:10.1016/j.jpeds.2011.11.040
- Lougee L, Perlmutter SJ, Nicolson R, Garvey MA, Swedo SE: Psychiatric disorders in first-degree relatives of children with pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS). J Am Acad Child Adolesc Psychiatry 39:1120–1126, 2000.
- Zibordi, Federica et al. CANS: Childhood acute neuropsychiatric syndromes. European Journal of Paediatric Neurology, Volume 22, Issue 2, 316 – 320