
27th October 2019. Dr Chee L Khoo
In medicine, newer is usually better although sometimes, we can be sceptical whether “newer” means a sneaky way to extend patents. The newer, second generation insulins, Toujeo® (insulin glargine U300 or GLA-300) and Degludec® are truly better insulins. Diabetes Therapy recently published a practical guide to the use of these second generation insulins (1). I highly recommend this article not just because I am a listed co-author, but it provides a practical guide to their use in the management of patients with type 2 diabetes (T2D) in Australian primary care setting.
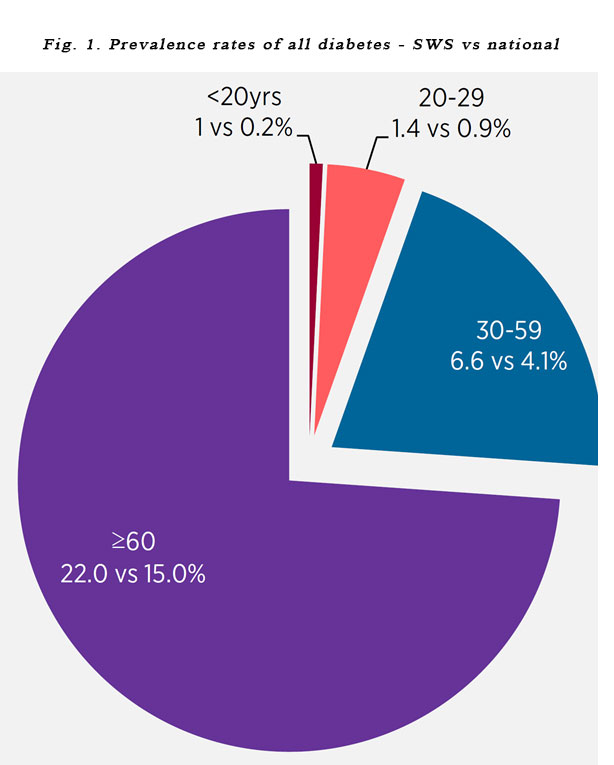
General practice is the principal point of care for the majority of patients with T2D. Data from Australian National Census, NDSS and NSW Adult Health survey 2017 indicate that the overall prevalence of diabetes in south west Sydney (SWS) is 6.7% compared with 5.3% and 5.1% for NSW and nationally respectively. Across all age groups, SWS has higher prevalence rates of all forms of diabetes compared with the rest of Australia (see Figure 1).
However, evidence shows that there is considerable clinical inertia in initiating insulin in face of deteriorating HbA1c. The inadequate training we all received in the use of insulin therapy in medical schools as well as during our resident years has meant that patients with T2D sit on suboptimal HbA1c for years before a decision is made to escalate treatment. Insulin was often initiated after HbA1c levels had remained between 8% and 9.3% for an extended period of time [2–4],This may stem from the physician’s and patient’s fear of hypoglycaemia and the perception of the complexity of initiation and titration.
In general, insulin therapy is required in:
- Type 1 diabetes
- Severe or symptomatic hyperglycaemia
- Diabetes in pregnancy
- Sepsis
- (Sometimes) in peri-operative care
- (Sometimes) in patients on corticosteroids
More commonly though, in primary care, insulin is frequently required when oral or non-insulin injectables fail to get our patient to glycaemic target. If the patient is on maximal oral therapy (triple or quadruple therapy), “see you in three months” just means you still have to deal with the problem in three months’ time. The earlier you initiate insulin when it is required, the easier it is as you still have significant beta cell function to assist in some of the post prandial insulin needs.
The newer second-generation insulin analogues provide an excellent option with their simple initiation regimen and a reduced risk of hypoglycaemia. Patients with T2D have different lifestyles and dietary habits and these new insulins can fit nicely into all sorts of lifestyles and dietary patterns. The pharmacodynamics of the newer insulins can assist the clinicians to support glycaemic management focussing on patient needs. They not only have longer duration of action, they achieve less glycaemic variability (a more even and flatter curve). They also have less intra-patient and less inter-patient differences.
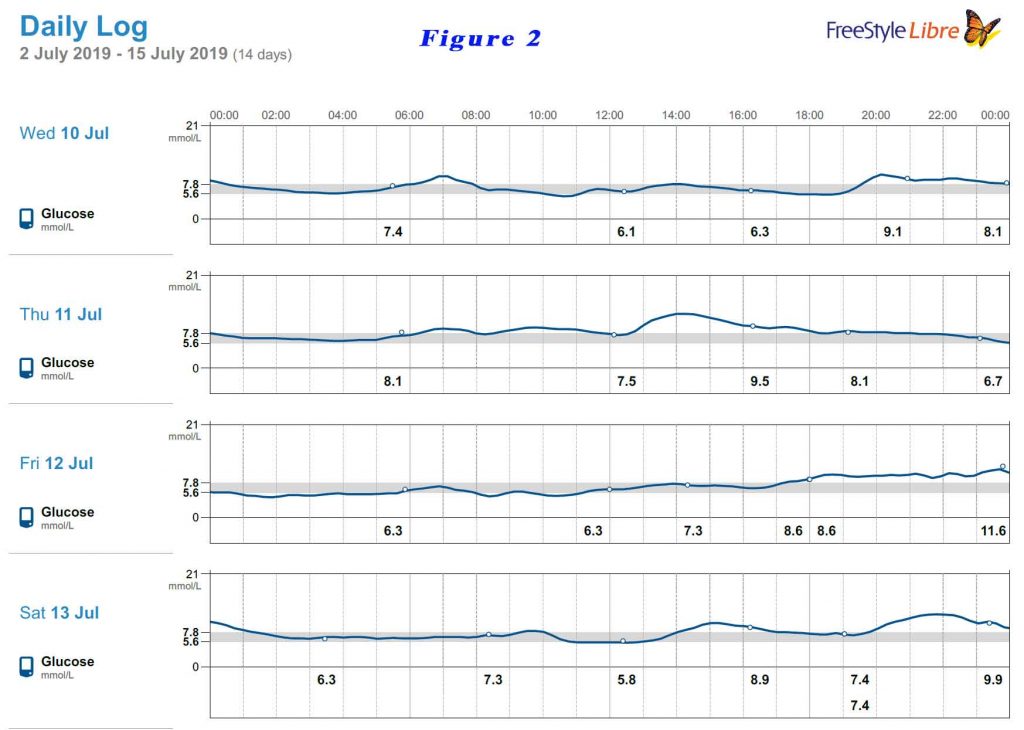
Have a look at this patient’s continuous glucose monitoring (CGM) profile. He is on basal insulin only but is on a very low carbohydrate diet. Thus, he does not have much prandial insulin requirements. See figure 2. Have you seen any glucose curve that is flatter than that?
Where is the evidence?
The “newer” second generation isn’t that “new” anymore. There is a comprehensive collection of clinical trials comparing GLA-300 to “older” insulins” and oral hypoglycaemic agents in a variety of populations of patients (5-8). These are the EDITION studies involving GLA-300. EDITION 1, 2 and 3 demonstrated lower rates of hypoglycaemic events and particularly nocturnal hypoglycaemia, positively comparing Gla-300 to Gla-100. EDITION 4 demonstrated comparable HbA1c levels between the two insulins.
We don’t have Degludec on its own in Australia but degludec comes with a prandial insulin in Ryzodeg® which is available on the PBS. In a review of randomised controlled trials comparing with Gla-300 and Degludec in patients with both type 1 and 2 diabetes [9], both insulins have as good as efficacy in lowering HbA1c with the older insulins but have significantly lower hypoglycaemic events (including the dreaded nocturnal hypoglycaemia) compared with older insulins.
The newer insulins offer a simple regimen to initiate insulin therapy. The titration algorithm is also very simple (see Figure 2). They do the job in achieving HbA1c targets but with less harm of hypoglycaemia.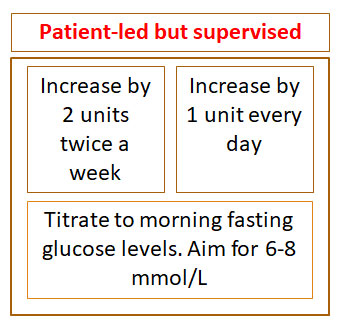
I recommend the 5-page article to you. It’s titled “Improving Type 2 Diabetes Management in General Practice Using a Second-Generation Basal Insulin Analogue Insulin Glargine 300U/mL: A Practical Guide” and is available as an open access article here.
Better still, come and join us on Sunday, 10th November at Mercure Hotel, Liverpool at the DMOTRU GP Diabetes Masterclass where practical cases will be workshopped. Each case simulates the types of patients we see in our everyday practice. You get to play with the insulin devices as well. Limited places are available. Click here for registration before it closes.
References:
- Deed, G., Rasalam, R., Khoo, C. et al. Improving Type 2 Diabetes Management in General Practice Using a Second-Generation Basal Insulin Analogue Insulin Glargine 300 U/mL: A Practical Guide Diabetes Ther (2019). https://doi.org/10.1007/s13300-019-00704-0
- Fulcher G, et al. What happens when patients require intensification from basal insulin? A retrospective audit of clinical practice for the treatment of type 2 diabetes from four Australian centres. Diabetes Res Clin Pract. 2015;108(3):405–13.
- Carrington MJ, Cohen N, Wiley JF. Blood glucose levels and glycaemic burden in 76,341 patients attending primary care: bittersweet findings from a 9-year cohort study. Diabetes Res Clin Pract. 2017;127:89–96.
- Khunti K, Millar-Jones D. Clinical inertia to insulin initiation and intensification in the UK: a focused literature review. Primary Care Diabetes. 2017;11(1):3–12.
- Ritzel R, et al. Patient-level meta-analysis of the EDITION 1, 2 and 3 studies: glycaemic control and hypoglycaemia with new insulin glargine 300 U/mL versus glargine 100 U/mL in people with type 2 diabetes. Diabetes Obes Metab. 2015;17(9):859–67.
- Yki-Jarvinen H, et al. Glycaemic control and hypoglycaemia with new insulin glargine 300 U/mL versus insulin glargine 100 U/mL in people with type 2 diabetes using basal insulin and oral antihyperglycaemic drugs: the EDITION 2 randomized 12-month trial including 6-month extension. Diabetes Obes Metab. 2015;17(12):1142–9.
- Bolli GB, et al. New insulin glargine 300 U/mL compared with glargine 100 U/mL in insulin-naïve people with type 2 diabetes on oral glucose-lowering drugs: a randomized controlled trial (EDITION Diabetes Obes Metab. 2015;17(4):386–94.
- Riddle MC, et al. New insulin glargine 300 units/mL versus glargine 100 units/mL in people with type 2 diabetes using basal and mealtime insulin: glucose control and hypoglycemia in a 6-month randomized controlled trial (EDITION 1). Diabetes Care. 2014;37(10):2755–62.
- Woo VC. A review of the clinical efficacy and safety of insulin degludec and glargine 300 U/mL in the treatment of diabetes mellitus. Clin Ther. 2017;39(82):S12–33.