
26th January 2022, Dr Chee L Khoo
How many reps have you seen recently promoting their bronchodilators? It’s all very confusing to me with the LAMA/LABA combo and now they have inhaled corticosteroids in the triple combo puffers. Who are these puffers for? Initially, they suggest triple therapy for COPD but they are now recommending the same for patients with severe asthma if the traditional LABA/ICS combo is not controlling the asthma. What if patients with severe asthma continue to have persistent symptoms or frequent exacerbations despite triple therapy? We need to consider biologic therapies but what are these biologic therapies? Who are they for? How do they work?
Asthma that is difficult to treat is considered to be severe when control remains poor despite measures that adequately address each of these three variables – regular inhaled corticosteroids, inhaler techniques and treatment of “irritants” including allergens. Up to 10% of adults and 2.5% of children with asthma have severe asthma, with a reduced quality of life and an increased risk of fixed airflow limitation, exacerbations, health care resource use, hospitalisation, and death. Patients with severe asthma have persistent symptoms or frequent exacerbations that require repetitive glucocorticoid bursts, maintenance oral glucocorticoid therapy, or both, despite adequate treatment with high-dose inhaled glucocorticoids, long-acting β2-agonists and long-acting muscarinic antagonists (1).
Not all patients with severe asthma are the same. Severe asthma is a heterogeneous syndrome encompassing different phenotypes depending on a number of different elements:
- Age at the onset of asthma (onset in childhood vs onset in adulthood)
- Presence or absence of allergy and other coexisting conditions
- Severity of airflow limitation,
- Frequency of exacerbations,
- Response to treatment and
- Prognosis
There are two different biological type of severe asthma – type 2 high inflammation and type 2 low inflammation. Type 2 high-inflammation (type 2–high) asthma is characterised by eosinophilic airway inflammation which is associated with increased blood eosinophil counts or elevations of fractional exhaled nitric oxide (Feno). Approximately 50% of cases of mild-to-moderate asthma and probably a larger proportion of cases of severe asthma are type 2–high asthma (2,3). The culprit triggers of type 2 – high asthma are usually allergens, pollutants, virus or bacteria. Type 2–high eosinophilic airway inflammation is present in allergic asthma, most frequently starting in childhood (i.e., childhood onset asthma), and in adult-onset, severe eosinophilic asthma (which is less often associated with allergy).
Type 2 low-inflammation (type 2–low) asthma encompasses neutrophilic asthma and pauci-granulocytic asthma. There are some patients with coexistence of eosinophilic and neutrophilic airway inflammation characterises mixed granulocytic asthma.
The inflammatory response in severe asthma
There are different pathways leading to airway inflammation in severe asthma. Different biological agents target different pathways depending on which pathways are triggered in that patient with severe asthma.
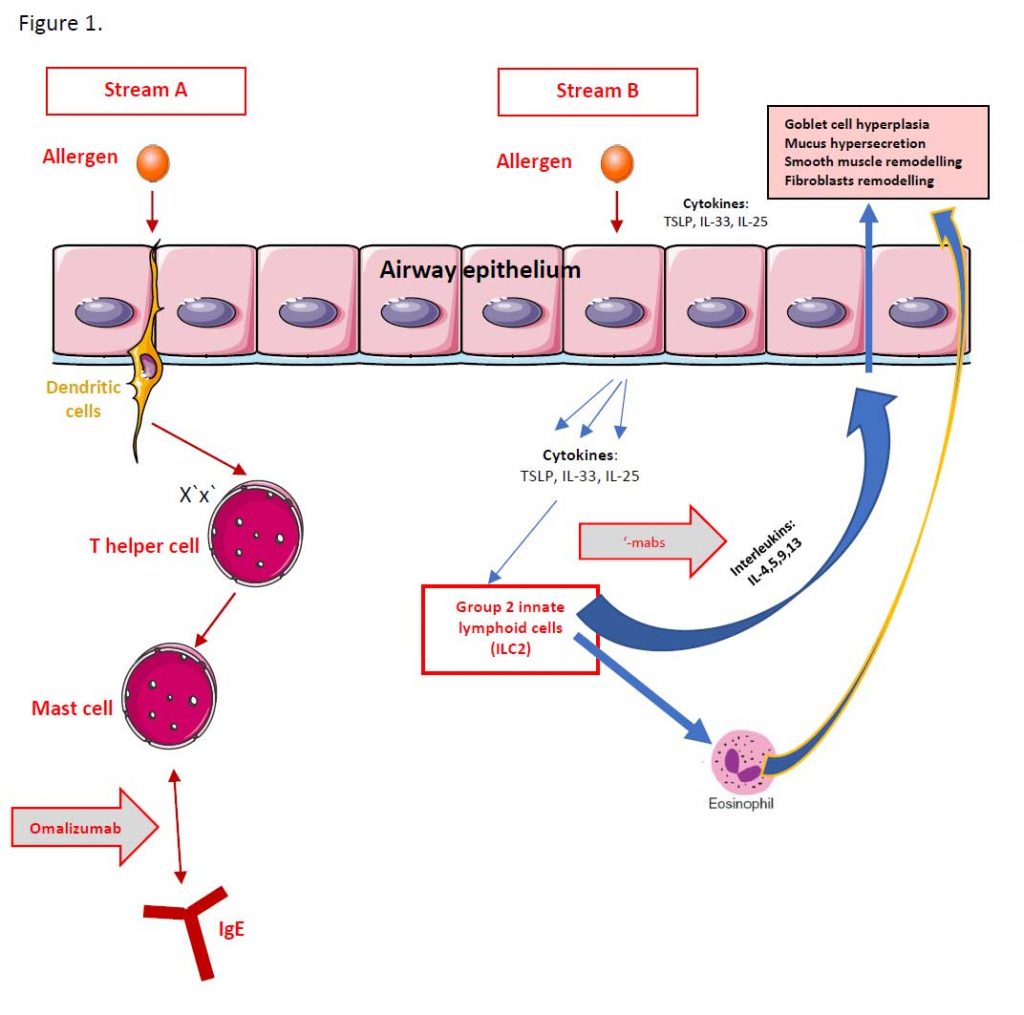
In some patients who have severe asthma and allergies, inhaled allergens trigger off a cascade of inflammatory responses starting from trans-membrane dendritic cells to mast cells and activating T-helper cells and ultimately, IgE antibodies. Inflammatory mediators identified include interleukin 3, 4, 5, 25, 23 and thymic stromal lymphopoietin (TSLP). These are patients with evidence of other allergies like nasal polyposis.
Omalizumab is an anti-IgE monoclonal antibody and has been shown to reduce free IgE levels in serum and inhibits binding of IgE to its high-affinity receptor on mast cells and basophils. It is used in persons 6 years of age or older who have moderate-to-severe allergic asthma, with a positive skin-prick test or allergen-specific IgE to a perennial aeroallergen, and whose symptoms are not controlled by inhaled glucocorticoids. A review assessing 25 clinical trials concluded that omalizumab reduced asthma exacerbations and hospitalisations, with small improvements in quality of life and lung function (4).
In a post hoc analysis, reductions in asthma exacerbations were greater in subgroups of patients with high Feno, blood eosinophil levels, and serum periostin levels than in subgroups with low values (5). However, identification of biomarkers that accurately predict a therapeutic response to omalizumab is still warranted (6). See Stream A in Figure 1.
In other patients with severe asthma, in response to allergen exposure, airway epithelial cells release cytokines like thymic stromal lymphopoietin (TSLP), IL-33 and IL-25 which in turn activate group 2 innate lymphoid cells (ILC2). ILC2 then releases copious amounts of other interleukins (IL-4,5,9,13) which promote airway remodelling, goblet cell hyperplasia, mucus hypersecretion, smooth muscle and fibroblast remodelling. ILC2 also activates eosinophils which add further to the effect on the airways. See stream B in Figure 1
Mepolizumab and reslizumab, humanized monoclonal antibodies targeting the ligand IL-5, and benralizumab, which depletes eosinophils by binding to the interleukin-5 receptor (IL-5R). Although initial studies, which enrolled patients who had moderate asthma without evidence of eosinophilic airway subsequent investigator-initiated trials showed significant reductions in exacerbations among patients with severe eosinophilic asthma (7,8).
Dupilumab (anti-IL-4Rα) is effective and is approved by the FDA for the treatment of atopic dermatitis and chronic rhinosinusitis with nasal polyposis, both of which are driven by type 2 inflammation. Thus, dupilumab is a convenient treatment for patients with either of these conditions and severe asthma.
Our understanding of the inflammatory pathways in patients with severe asthma has advanced greatly over the last few decades. There are more than one phenotypes of patients with severe asthma with different activated pathways. Some of these patients have a major involvement of IgE, some have elevated eosinophil counts (blood and airway) while others have elevated neutrophils (type 2 low inflammation). There are no biologic treatments available for type 2 low inflammation severe asthma yet.
A number of biological agents are now available for some patients with type 2 high severe asthma. These agents represent major breakthroughs significantly decreasing exacerbation rates and improving the quality of life and asthma control for patients with type 2–high severe asthma.
RCTs involving patients with oral glucocorticoid–dependent severe asthma have shown that addon therapy with mepolizumab, benralizumab, or dupilumab is glucocorticoid-sparing and reduces exacerbation rates. The ultimate aim is to prevent both short-term and long-term oral glucocorticoid use in people with severe asthma.
Thus, if you have patients with severe asthma who are still not adequately controlled on triple therapy, perhaps, it’s time to refer them to your favourite immunologist.
References:
- Global Initiative for Asthma. 2021 GINA report, global strategy for asthma management and prevention (2021 update) (https://ginasthma .org/gina-reports)
- Woodruff PG, Modrek B, Choy DF, et al. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am J Respir Crit Care Med 2009; 180: 388-95.
- Frossing L, Silberbrandt A, Von Bulow A, Backer V, Porsbjerg C. The prevalence of subtypes of type 2 inflammation in an unselected population of patients with severe asthma. J Allergy Clin Immunol Pract 2021; 9: 1267-75.
- National Institute for Health and Care Excellence. Omalizumab for treating severe persistent allergic asthma. 2013 https://www .nice.org.uk/guidance/ta278
- Hanania NA, Wenzel S, Rosen K, et al. Exploring the effects of omalizumab in allergic asthma: an analysis of biomarkers in the EXTRA study. Am J Respir Crit Care Med 2013; 187: 804-11.
- Casale TB, Luskin AT, Busse W, et al. Omalizumab effectiveness by biomarker status in patients with asthma: evidence from PROSPERO, a prospective real-world study. J Allergy Clin Immunol Pract 2019; 7(1): 156-164.e1.
- Nair P, Pizzichini MMM, Kjarsgaard M, et al. Mepolizumab for prednisone dependent asthma with sputum eosinophilia. N Engl J Med 2009; 360: 985-93.
- Haldar P, Brightling CE, Hargadon B, et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N Engl J Med 2009; 360: 973-84.
- Brusselle GG, Koppelman GH. Biologic Therapies for Severe Asthma. N Engl J Med. 2022 Jan 13;386(2):157-171. doi: 10.1056/NEJMra2032506. PMID: 35020986.
- Salter BM, Aw M, Sehmi R. The role of type 2 innate lymphoid cells in eosinophilic asthma. J Leukoc Biol. 2019 Oct;106(4):889-901. doi: 10.1002/JLB.3MR1217-497R. Epub 2019 May 7. PMID: 31063647.