
12th July 2026, A/Prof Chee L Khoo

We don’t see many acute pancreatitis in our rooms but the incidence of acute pancreatitis is gradually increasing (1). Many will develop further episodes and some will develop chronic pancreatitis. Although most patients with acute pancreatitis have its mild form, some develop moderate or severe acute pancreatitis, both of which include serious complications and an increased risk for death. The four most common causes of acute pancreatitis are gallstones (40%), heavy alcohol use (30%), hypertriglyceridemia (2%-7%), and certain medications (< 5%) (2). The US FDA has just approved olezarsen to reduce triglyceride levels and the risk of acute pancreatitis in adults with severe hypertriglyceridaemia.
Before we can look at what olezarsen is, we need to re-look at triglyceride metabolism.
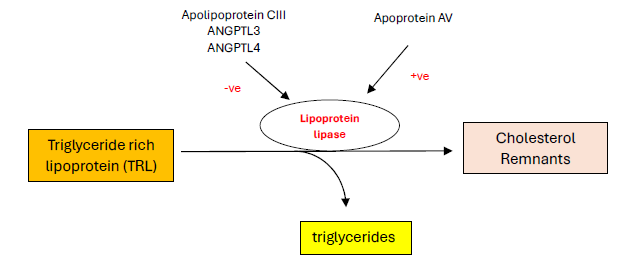
Triglyceride-rich lipoproteins (TRL) are a class of lipoproteins that contain a high proportion of triglycerides. The main types of TRL are chylomicrons and VLDL. Triglycerides (TG) are cleaved off the TRL by endothelial surface located lipoprotein lipase (LL) leaving behind TG rich remnants. LL is negatively impacted by a number of factors including apolipoprotein CIII (apoCIII). ApoCIII blocks LL which inhibits the cleaving of TG inducing hypertriglyceridaemia. See Figure 1.
Olezarsen is an antisense oligonucleotide which blocks apoCIII and reduces triglycerides. Olezarsen is not entirely new. It was approved in 2024 as an adjunct to diet for adults living with familial chylomicronemia syndrome (FCS), based on results of the phase 3 BALANCE trial.
FCS is an inherited autosomal recessive disorder affecting approximately 1–2 individuals per million. It disrupts the normal breakdown of triglycerides carried by chylomicrons. Most commonly, FCS results from mutations in the LPL gene, which encodes lipoprotein lipase, an enzyme essential for breaking down triglycerides.
In the BALANCE trial, 66 patients with FCS were randomised to receive either 80mg of olazarsen, 50mg of olazarsen or placebo (3). The baseline TG level were ~30mmol/L and 71% had history of acute pancreatitis in the previous 10 years.
At 6 months, the difference in the mean percent change in the apolipoprotein C-III level from baseline to 6 months in the 80-mg group as compared with the placebo group was −73.7 percentage points (95% CI, −94.6 to −52.8) and between the 50-mg group as compared with the placebo group was −65.5 percentage points (95% CI, −82.6 to −48.3). By 53 weeks, 11 episodes of acute pancreatitis had occurred in the placebo group, and 1 episode had occurred in each olezarsen group (rate ratio [pooled olezarsen groups vs. placebo], 0.12; 95% CI, 0.02 to 0.66).
The new indication under the FDA came from data from two randomised, double-blind, placebo-controlled phase 3 trials — CORE-TIMI 72a and CORE2-TIMI 72b — involving more than 1000 adults with severe hypertriglyceridemia (4). 1061 patients with severe hypertriglycerides were randomised to either 50mg olezarsen,, 80mg olezarsen or placebo. The median triglyceride level at baseline was 8.96 mmol/L (range: 6.71 to 14.11 mmol/L) across both trials.
At 6 months, the mean change from baseline in the triglyceride level was −62.9 percentage points in the olezarsen 50-mg group and −72.2 percentage points in the olezarsen 80-mg group in the CORE-TIMI 72a trial and was −49.2 percentage points in the olezarsen 50-mg group and −54.5 percentage points in the olezarsen 80-mg group in the CORE2-TIMI 72b trial (P<0.001).
During 696.1 patient-years in the pooled olezarsen group, 7 acute pancreatitis events occurred in 5 of 705 patients (observed incidence rate: 1.01 events per 100 patient-years). During 352.9 patient-years in the pooled placebo group, 22 acute pancreatitis events occurred in 17 of 356 patients (observed incidence rate: 6.23 events per 100 patient-years). The mean rate ratio for acute pancreatitis with olezarsen as compared with placebo was 0.15 (p<0.001).
Up until now, we don’t really have effective agents that substantially reduce triglyceride levels in patients with severe hypertriglyceridaemia. Fenofibrate or omega-3 fish oil capsules just aren’t potent enough to cause meaningful reductions in triglycerides in patients with severe hypertriglycerides (>5.5mmol/L) to prevent acute pancreatitis.
The primary purpose of triglyceride lowering in patients with severe hypertriglyceridemia is to reduce the risk of acute pancreatitis, which can be life-threatening. Current therapies have more modest triglyceride-lowering effects in patients with severe hypertriglyceridemia and have not been shown to reduce the incidence of pancreatitis in this population.
References:
- Iannuzzi J, King J, Leong J et al. Global Incidence of Acute Pancreatitis Is Increasing Over Time: A Systematic Review and Meta-Analysis. Gastroenterology, 2021; 162, 122-134
- Trikudanathan G, Yazici C, Evans Phillips A et al. Diagnosis and Management of Acute Pancreatitis. Gastroenterology, 2024; 167, 673-688
- Stroes ESG, Alexander VJ, Karwatowska-Prokopczuk E, Hegele RA, Arca M, Ballantyne CM, Soran H, Prohaska TA, Xia S, Ginsberg HN, Witztum JL, Tsimikas S; Balance Investigators. Olezarsen, Acute Pancreatitis, and Familial Chylomicronemia Syndrome. N Engl J Med. 2024 May 16;390(19):1781-1792.
- Marston NA, Bergmark BA, Alexander VJ, et al. CORE-TIMI 72a and CORE2-TIMI 72b Investigators. Olezarsen for Managing Severe Hypertriglyceridemia and Pancreatitis Risk. N Engl J Med. 2026 Jan 29;394(5):429-441.