
28th June 2026, A/Prof Chee L Khoo
It’s all over the news. Teplizumab (Tzield) has just been approved by the Australian Therapeutic Goods Administration (TGA) delay the onset of Stage 3 type 1 diabetes mellitus (T1D) in adult and paediatric patients aged 8 years and older with Stage 2 type 1 diabetes mellitus (1). Wow. But what does that mean for our patients already with T1D or those who are at very high risk of developing T1D? Nope. Not helpful for those already with T1D (i.e. Stage 3 or Stage 4 – see below). Who are the Stage 2 T1D patients? We better go back to the drawing board to clarify what the stages of T1D all mean.
It’s been 5 years since we review the efforts in prevention of T1D. A lot has happened in the space since then. They were talking about the three stages of T1D. There is a fourth stage now. The stages of T1D inform us of the progression of the disease. Essentially, The International Society for Pediatric and Adolescent Diabetes (ISPAD) guidelines described the four stages of T1D:
- Stage 1 – ≥ 2 islet autoantibodies (AABs), normoglycemia and asymptomatic
- Stage 2 – ≥ 2 islet AABs, elevated fasting glucose or impaired glucose tolerance (IGT) on oral glucose tolerance test (OGTT), HbA1c 5.7–6.5%, or ≥10% change in HbA1c
- Stage 3 – This is your usual T1D – full hyperglycaemia. May be symptomatic or asymptomatic
- Stage 4 – Long-standing T1D, likely with complications (2)
Children with a single islet AAB do not have T1D but are considered “at risk”. But not all patients with single ABB progress to Stage 3 TID. The 15-year risk of diabetes in this population was 0·4% when no islet autoantibodies were present, 12·7% when 1 was present (3).
Clinically available islet ABBs that have been tested include:
- Glutamic acid decarboxylase Antibody
- Insulinoma antigen-2 (IA-2)
- Insulin autoantibody (IAA)
- zinc transporter 8 (ZnT8)
The primary goals of monitoring people with early-stage (pre-symptomatic Stages 1 & 2) T1D are to
- Reduce the acute presentation of T1D when first diagnosed. Prevent DKA – complications from DKA are linked to poorer long term outcomes
- prepare patient and carers of the impending disease, smooth the transition at diagnosis of clinical T1D with early education and support
- enable ready access to disease modifying therapy either in trials, or eventually as part of routine care
Progression
Data informing us of the progression of the stages of T1D were primarily obtained from birth and early life cohorts (ie, Diabetes Autoimmunity Study in the Young [DAISY], Type 1 Diabetes Prediction and Prevention [DIPP], BABYDIAB, and BABYDIET) that combined genetic screening with islet autoantibody testing and metabolic information (3).The more positive AABs there are, the more likely the progression to Stage 3 T1D.
Primarily from those data, people with a first-degree relative with T1D have up to a 15X increased risk of developing T1D compared to persons without a known family history of T1D []. The vast majority (>70%) of young people with multiple islet AABs progress to Stage 3 within 15 years, compared to only 15% who have a single islet AABs. Thus, people with two or more islet AABs have early-stage T1D and should no longer be referred to as being “at risk for T1D”.
Limitations of the current model
The progression figures we quoted above are based on a set population pooled from a number of studies but as more data comes in, the numbers will be different. There is a wide variability of risk within a single stage. The risk of progression or not is affected by:
- Type of positive islet AABs
- Age of the people tested
- Presence or absence of different genes
- The metabolic profile of the people at different stages and age of the testing
Which islet AABs?
The presence of insulinoma-associated protein 2 autoantibodies (IA2A) as one of the multiple autoantibodies can sway the risk for disease widely compared with combinations lacking IA2A. Specifically, the 5-year risk for progression from stage 1 to stage 3 jumps to 60% with this particular autoantibody, versus 21% when it is absent (4). The current staging system does not account for this distinction.
While most individuals with a single AAB do not progress to stage 3, if the positive AAB is IA2A (which is uncommon as a single autoantibody), the risk of progression to stage 3 is 2-4X greater than the presence of GADA alone (5,6).
In DAISY, the 10-year risk in individuals with single autoantibody positivity was 14·5%, an observation largely driven by those with IA2A, for whom 40·5% developed type 1 diabetes and only 12·9% with single GADA positivity and 13·1% with single insulin autoantibodies (IAAs) developed clinical type 1 diabetes (3).
Further, when thresholds of combined glucose and C-peptide measures considered together, the risk of progression to clinical disease is much more imminent than when criteria based on dysglycaemia (a glucose-only measure) or HbA1c are used without consideration of the C-peptide (7-10).
Teplizumab is a humanised monoclonal antibody to CD3 on T cells. In a Phase 3 randomised, placebo-controlled trial, 217 children and adolescents aged ≥ 8 years old with Stage 2 TID (i.e. preclinical T1D – before dysglycaemia) were randomised to receive intravenous teplizumab or matching placebo for two 12-day courses. At 78 weeks, patients treated with teplizumab had significantly higher stimulated C-peptide levels than patients receiving placebo (111 patients) (14). 94.9% of patients treated with teplizumab maintained a clinically meaningful peak C-peptide level of 0.2 pmol/ml or greater, as compared with 79.2% of those receiving placebo.
So, who do we screen?
Thus, it is not that straightforward when we test potential people for islet antibodies. On one hand, we do want to find those who are at high risk of progression to Stage 3 TID including those that are imminent but we don’t to alarm those who only have one positive islet ABB which may or may not progress to Stage 3 TID. There may be a lot of unnecessary psychological distress.
The next issue is then who should we screen. Until recently, most screening programs focused on those with a family history of T1D. While family history-based screening markedly increases per-test probability of identifying people with islet AABs, it fails to identify 90% of those who will ultimately develop T1D. A significant proportion of people who have T1D do not have a family history of T1D. Thus, screening based on family history will miss a majority of at-risk people.
Programs such as the Global Platform for the Prevention of Autoimmune Diabetes (GPPAD), Fr1da, Autoimmunity Screening for Kids (ASK), Population Level Estimate of T1D Risk Genes in Children (PLEDGE), Combined Antibody Screening for Celiac and Diabetes Evaluation (CASCADE), the Australian T1D National Screening Pilot, and the TRIAD study continue to demonstrate the feasibility of general population and genetic risk stratified screening and follow-up programs [9-11]. We are not there yet.
When do we screen?
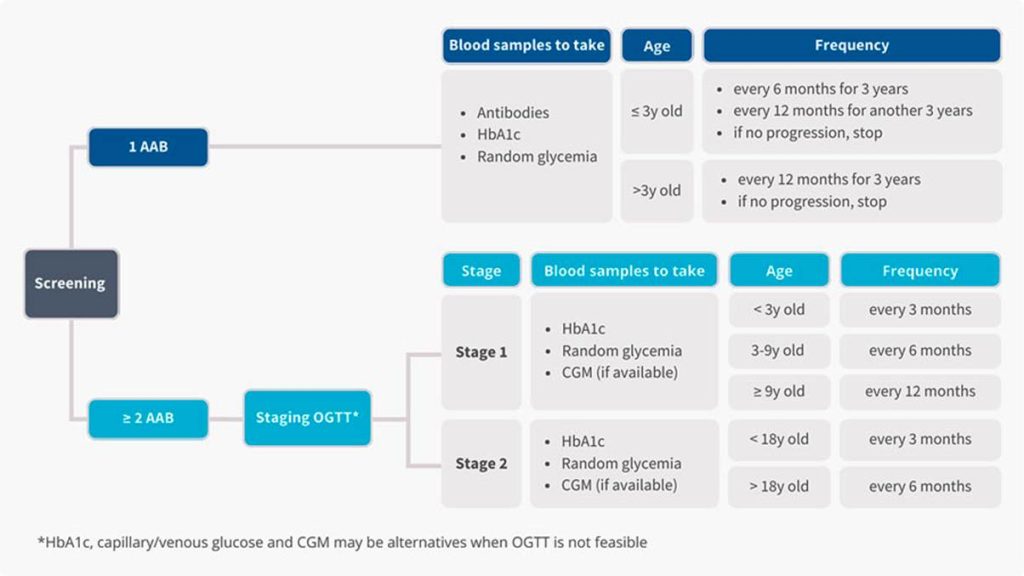
Not everyone with 2 islet ABBs will progress. So, who do we investigate and when do we repeat those investigations? While our data is evolving, there is preliminary recommendations on further investigations and follow up testing in those found to have positive islet ABBs (12, 13) – see Figure 1:
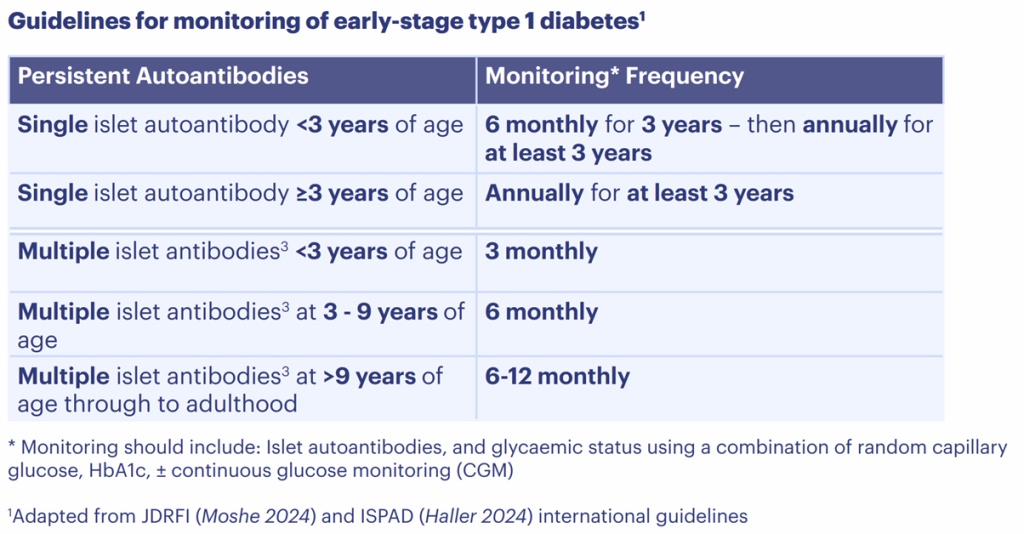
We don’t have screening or follow up guidelines in Australia yet but the International Society for Pediatric and Adolescent Diabetes (ISPAD) 2024 guidelines is a step forward (13) – see Figure 2:
Around half of clinical type 1 diabetes diagnoses occur in adulthood. Some of these adults may have already developed multiple islet autoantibodies in childhood or adolescence, but it is likely that many would be missed (islet autoantibody negative) if they had been screened during childhood. The algorithm in early diagnosis is adults is even more complicated.
In the meantime, if there is a close relative with T1D, perhaps, a referral to a endocrinologist who is up to date with current guidelines will be a good idea.
References:
- https://www.tga.gov.au/resources/auspmd/tzield-teplizumab. Accessed 11/06/2026
- Haller MJ, Bell KJ, Besser REJ, Casteels K, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Screening, Staging, and Strategies to Preserve Beta-Cell Function in Children and Adolescents with Type 1 Diabetes. Horm Res Paediatr. 2024;97(6):529-545.
- Ziegler AG, Rewers M, Simell Oet al. Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA. 2013 Jun 19;309(23):2473-9.
- Jacobsen LM, Bocchino L, Evans-Molina C, et al. The risk of progression to type 1 diabetes is highly variable in individuals with multiple autoantibodies following screening. Diabetologia 2020; 63: 588–96
- Sims EK, Cuthbertson DD, Bosi E, et al. Single islet antigen 2 antibody–positive (IA2A Ab+) children exhibit significant metabolic abnormalities and 5-year type 1 diabetes (T1D) risk. Diabetes 2023; 72 (suppl 1): 1440–P.
- Achenbach P, Warncke K, Reiter J, et al. Stratification of type 1 diabetes risk on the basis of islet autoantibody characteristics. Diabetes 2004; 53: 384–92
- Sosenko JM, Skyler JS, Mahon J, et al. Use of the Diabetes Prevention Trial-Type 1 Risk Score (DPTRS) for improving the accuracy of the risk classification of type 1 diabetes. Diabetes Care 2014; 37: 979–84
- Sims EK, Cuthbertson DD, Bosi E, et al. Index60 stratification enhances current staging for type 1 diabetes by identifying at-risk single islet autoantibody positive (Ab+) individuals. Diabetes 2023; 72 (suppl 1): 1441–P (abstr).
- Naredi Scherman M, Lind A, Hamdan S, Lundgren M, Svensson J, Pociot F, et al. Home capillary sampling and screening for type 1 diabetes, celiac disease, and autoimmune thyroid disease in a Swedish general pediatric population: the TRIAD study. Front Pediatr. 2024;12:1386513.
- Hendriks AEJ, Marcovecchio ML, Besser REJ, Bonifacio E, Casteels K, Elding Larsson H, et al. Clinical care advice for monitoring of islet autoantibody positive individuals with presymptomatic type 1 diabetes. Diabetes Metab Res Rev. 2024;40(2):e3777.
- Sims EK, Besser REJ, Dayan C, Geno Rasmussen C, Greenbaum C, Griffin KJ, et al. Screening for type 1 diabetes in the general population: a status report and perspective. Diabetes. 2022;71(4):610–23
- Phillip M, Achenbach P, Addala A, et al. Consensus Guidance for Monitoring Individuals With Islet Autoantibody-Positive Pre-Stage 3 Type 1 Diabetes. Diabetes Care. 2024 Aug 1;47(8):1276-1298.
- Haller MJ, Bell KJ, Besser REJ, et al. ISPAD Clinical Practice Consensus Guidelines 2024: Screening, Staging, and Strategies to Preserve Beta-Cell Function in Children and Adolescents with Type 1 Diabetes. Horm Res Paediatr. 2024;97(6):529-545. doi: 10.1159/000543035. Epub 2024 Dec 11. PMID: 39662065; PMCID: PMC11854978
- Ramos EL, Dayan CM, Chatenoud L, Sumnik Z, Simmons KM, Szypowska A, Gitelman SE, Knecht LA, Niemoeller E, Tian W, Herold KC; PROTECT Study Investigators. Teplizumab and β-Cell Function in Newly Diagnosed Type 1 Diabetes. N Engl J Med. 2023 Dec 7;389(23):2151-2161.