
10th May 2026, A/Prof Chee L Khoo

We were taught in medical school that meniscal injuries inevitably need arthroscopic debridement. Of course, these are likely the ones that don’t improve with physical therapy – physiotherapy, hydrotherapy or chiropractic treatment. We don’t see those that got better with conservative measures. We also don’t see what happen after they had arthroscopic debridement. Do they get better? Are they better than conservative measures? Once you get passed 50 years old, the system frown upon the surgeon operating on these meniscal tears because the “long term” results are the same whether the menisci are trimmed or not. They all end up with a knee replacement down the track.
Patients can tear their menisci after a traumatic injury. This is commonly the case in younger patients in sporting or work injuries. The forces involved are usually substantial. More than likely, these will need debridement even though these are stronger patients.
Even without significant trauma, as we get older, the menisci can degenerate and tears can occur purely from ordinary wear and tear. There may be minor twisting injuries from a fall or a stumble which the patient may often not remember. These “injuries” are what we see in primary care when patient presents with knee pain and we blame them on “arthritis”.
Many of our older patients with knee pains will have coexisting osteoarthritis. Often, an MRI is organised and inevitably, a meniscal tear will be demonstrated. Some evidence of osteoarthritis is generally present. These are our degenerative menisci rather than traumatic torn menisci. Nonetheless, these patients continue to be symptomatic “despite physiotherapy” and arthroscopic debridement is often recommended. It is logical to think that trimming the menisci will improvement symptoms.
Will arthroscopic debridement of menisci in patients without osteoarthritis help with symptoms improvement?
Sihvonen et al conducted a multicentre, randomised, double-blind sham-controlled trial in 2013 to assess the efficacy of arthroscopic partial meniscectomy in patients who have a degenerative tear of the medial meniscus without knee osteoarthritis (1). It was a small trial with 146 participants aged 35 – 65 years who had knee pain for >3 months that was unresponsive to conservative treatment and had clinical findings consistent with a tear of the medial meniscus. The participants were recruited from five orthopaedic clinics in Finland during the period from December 2007 through January 2013. Participants with a traumatic onset of symptoms or radiographic criteria of osteoarthritis are excluded.
The randomisation was most interesting. Preoperative magnetic resonance imaging (MRI) was performed to confirm the presence of a medial meniscus tear, but the eligibility of the patients was ultimately determined by arthroscopic examination. At the start of the operation and when osteoarthritis is excluded and a meniscal tear is confirmed, the surgeon asked a research nurse to open an envelope containing the study-group assignment (arthroscopic partial meniscectomy or sham surgery) and reveal it to the surgeon; the assignment was not revealed to the patient.
For patients randomised to undergo meniscectomy, the usual comprehensive arthroscopic meniscectomy is performed. For the sham surgery, a standard arthroscopic partial meniscectomy was simulated. The same instruments are requested and used but no meniscal trimming is performed. The patient was also kept in the operating room for the amount of time required to perform an actual arthroscopic partial meniscectomy.
Only the orthopaedic surgeon and other staff in the operating room were made aware of the group assignment, and they did not participate in further treatment or follow-up of the patient. All patients receive the same walking aids and instructions for the same graduated exercise program.
Outcome measures
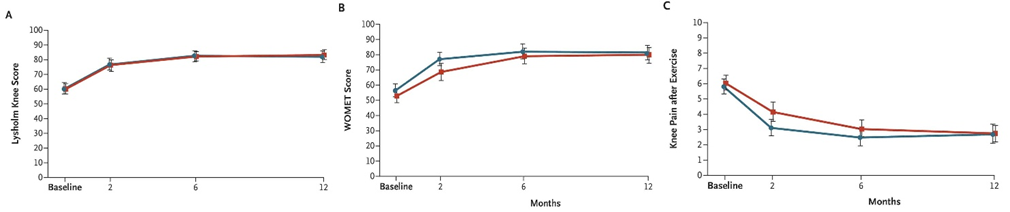
Primary outcomes were knee pain after exercise (during the preceding week), the Lysholm knee score and the Western Ontario Meniscal Evaluation Tool (WOMET) at 12 months after surgery. Knee pain was assessed on an 11-point scale ranging from 0 (no pain) to 10 (extreme pain). Both the Lysholm knee score and WOMET are a validated knee and meniscus-specific health-related quality-of-life scores respectively (2,3). The trial was designed to ascertain whether arthroscopic partial meniscectomy is superior to sham surgery, at 12 months after the procedure, with regard to the three primary outcomes.
Results
Although marked improvement from baseline to 12 months was seen in the three primary outcomes in both study groups, there were no significant between-group differences in the change from baseline to 12 months in any of these measures. In other words, surgery was no better than physical therapy at the end of 12 months. See Figure 1.
Implications of this trial
It was logical to think that in our patients with knee osteoarthritis whereby the articular cartilage has worn out and probably have holes in them, shaving the articular cartilage would smoothen the surface and relieve symptoms. Well, two clinical trials have put that logic to bed. The two controlled trials showed a lack of efficacy of arthroscopic surgery (4,5). The number of arthroscopic surgical procedures performed to treat established knee osteoarthritis, with or without a concomitant meniscal lesion, has decreased dramatically in the past 15 years (6,7).
What about those with osteoarthritis and concomitant torn menisci? Maybe, it’s the irregular menisci that were causing the pain. What if we just trim the menisci? Surely, that will improve knee pain symptoms. In trials that assessed the benefit of arthroscopic partial meniscectomy in the treatment of a degenerative meniscal tear in patients with varying degrees of knee osteoarthritis (8-10), arthroscopic surgery and exercise therapy were not superior to exercise therapy alone.
The 2013 clinical trial tested the logic of trimming the menisci in patients with knee pain but without knee osteoarthritis. Sihvonen et al have shown that trimming the menisci in these patients also isn’t any better than exercise alone.
Shivonen et al recently provided a 10 year update in a correspondence letter in the NEJM and showed that arthroscopic partial meniscectomy offers no benefits for degenerative meniscal tears even after 10 years and may worsen outcomes, with higher rates of osteoarthritis and knee surgeries compared to sham procedures (16).
In patients with knee pain with or without evidence of osteoarthritis, the pain is an early sign of knee osteoarthritis and not from the degenerate meniscus (11-14). One study showed no significant association between the presence of meniscal damage and the development of frequent knee pain in middle-aged and older adults, once the co-occurrence of osteoarthritis at baseline was taken into account (15).
Beyond the first few weeks of physiotherapy, exercise therapy (from an exercise physiologist) to regain muscle strength and alignment and patience can get our patients back to reasonable function. It will take at least 12 months.
References:
- Sihvonen R, Paavola M, Malmivaara A, Itälä A, Joukainen A, Nurmi H, Kalske J, Järvinen TL; Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med. 2013 Dec 26;369(26):2515-24.
- Tegner, Y, Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res 1985;198:43-49
- Sihvonen, R, Jarvela, T, Aho, H, Jarvinen, TL. Validation of the Western Ontario Meniscal Evaluation Tool (WOMET) for patients with a degenerative meniscal tear: a meniscal pathology-specific quality-of-life index. J Bone Joint Surg Am 2012;94:e65-e65
- Moseley, JB, O’Malley, K, Petersen, NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 2002;347:81-88
- Kirkley, A, Birmingham, TB, Litchfield, RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 2008;359:1097-1107[Erratum, N Engl J Med 2009;361:2004.]
- Kim, S, Bosque, J, Meehan, JP, Jamali, A, Marder, R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am 2011;93:994-1000
- Holmes, R, Moschetti, W, Martin, B, Tomek, I, Finlayson, S. Effect of evidence and changes in reimbursement on the rate of arthroscopy for osteoarthritis. Am J Sports Med 2013;41:1039-1043
- Katz, JN, Brophy, RH, Chaisson, CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med 2013;368:1675-1684
- Herrlin, SV, Wange, PO, Lapidus, G, Hallander, M, Werner, S, Weidenhielm, L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surg Sports Traumatol Arthrosc 2013;21:358-364
- Yim, JH, Seon, JK, Song, EK, et al. A comparative study of meniscectomy and nonoperative treatment for degenerative horizontal tears of the medial meniscus. Am J Sports Med 2013;41:1565-1570
- Englund, M, Guermazi, A, Gale, D, et al. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med 2008;359:1108-1115
- Bhattacharyya, T, Gale, D, Dewire, P, et al. The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee. J Bone Joint Surg Am 2003;85:4-9
- Ding, C, Martel-Pelletier, J, Pelletier, JP, et al. Meniscal tear as an osteoarthritis risk factor in a largely non-osteoarthritic cohort: a cross-sectional study. J Rheumatol 2007;34:776-784
- Englund, M, Guermazi, A, Roemer, FW, et al. Meniscal tear in knees without surgery and the development of radiographic osteoarthritis among middle-aged and elderly persons: the Multicenter Osteoarthritis Study. Arthritis Rheum 2009;60:831-839
- Englund, M, Niu, J, Guermazi, A, et al. Effect of meniscal damage on the development of frequent knee pain, aching, or stiffness. Arthritis Rheum 2007;56:4048-4054
- https://www.nejm.org/doi/full/10.1056/NEJMc2516079. Accessed 10/5/2026