
25th May 2026, A/Prof Chee L Khoo

All of us have more than a few patients with essential hypertension (i.e. hypertension with no secondary causes) who remain hypertensive despite two or three anti-hypertensives. These are patients who are already on an ACE inhibitor (ACEi) or angiotensin receptor blocker (ARB) plus a calcium channel blocker (CCB) or a diuretic or both. A mineralocortical receptor antagonist (spironolactone) (MRA) has been suggested as the third agent rather than the traditional diuretic because of aldosterone blockade has other cardio-renal benefits in addition to BP lowering. Of course, the MRAs comes with their adverse effects which can limit their use. We now have a new kid on the block if the ACEi/ARB plus CCB doesn’t quite bring our patients’ BP to target. It’s an aldosterone receptor inhibitor (ASI).
Physiological
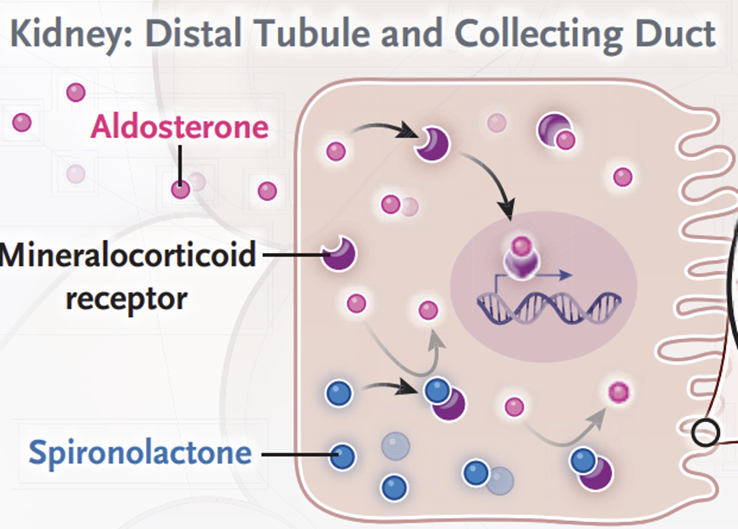
Before we go to look at this new class of medication, ASI, let’s look at what aldosterone do. It’s not just a diuretic. Aldosterone is synthesised in the zona glomerulosa of the adrenal gland and binds to mineralocortical receptors (MR). Aldosterone synthesis is triggered by:
- Angiotensin II
- Adrenocorticotropin (ACTH)
- Rise in serum potassium
- Stretch receptors in the atria and
- Lipid soluble factor(s) produced in fat tissue
Aldosterone secretion has been classically considered to be regulated by renin-angiotensin system (RAS) activation in response to intravascular volume contraction. When aldosterone binds to the MR, aldosterone increases reabsorption of sodium and excretion of potassium across renal tubular epithelial cells, leading to water retention, blood pressure rise and potassium excretion.
In disease states
In diverse disease states such as the cardiometabolic syndrome (CMS), heart failure and CKD, inappropriate aldosterone secretion occurs despite high salt and volume retention and contributes to a state of hyperaldosteronism. Elevated aldosterone in these disease states contributes to the pathophysiology of insulin resistance, endothelial dysfunction, glomerular hyperfiltration and excess glomerular and tubular leakage of albumin; processes that lead to maladaptive cardiovascular (left ventricular hypertrophy, cardiac fibrosis and diastolic dysfunction) and renal remodeling.
Adipose tissue produces a lipid soluble factor that stimulates aldosterone secretion (1). There is also emerging evidence that both aldosterone and glucocorticoids can interact via MRs to promote adipogenesis and increases in fat macrophage infiltration (1,2). Thus, the interaction of fat, the adrenal cortex, and aldosterone/glucocorticoids is a positive feedback relationship whereby fat increases aldosterone and glucocorticoid production, and these hormones, in turn, promote further adipogenesis and inflammation in fat tissue.
Data is also emerging that suggest patients with resistant hypertension, those not controlled to goal on three antihypertensive medications, tend to be overweight, often have elevated plasma and urine levels of aldosterone, and have salutary blood pressure responses to mineralocorticoid receptor (MR) blockers (2,3).
Aldosterone blockade
Steroidal MRAs (e.g. spironolactone, eplenerone) and non-steroidal MRAs (e.g. finerenone) counter these hyperaldosterone effects. However, their use as antihypertensives is constrained by hyperkalaemia, reduced safety and efficacy in advanced kidney disease, and sex hormone–related side effects (4). Because they block at the mineralo-receptor level, aldosterone levels remain high in circulation and patients on MRA therapy may remain at a high residual risk for poor outcomes even on MRA therapy. MRAs also trigger a compensatory increase in aldosterone with downstream consequences. See Figure 1.
Adapted from Tomasz J et al NEJM Oct 2025
What if we can directly block aldosterone synthesis?
We could inhibit aldosterone synthase which lead to reduce aldosterone production and thence, reduction in aldosterone levels in circulation. Earlier aldosterone synthase inhibitors (ASI) also block 11β-hydroxylase leading to cortisol suppression. See Figure 2. Thus, we now have selective aldosterone synthase inhibitors (ASI), baxdrostat and lorundrostat which do not suppress cortisol production.
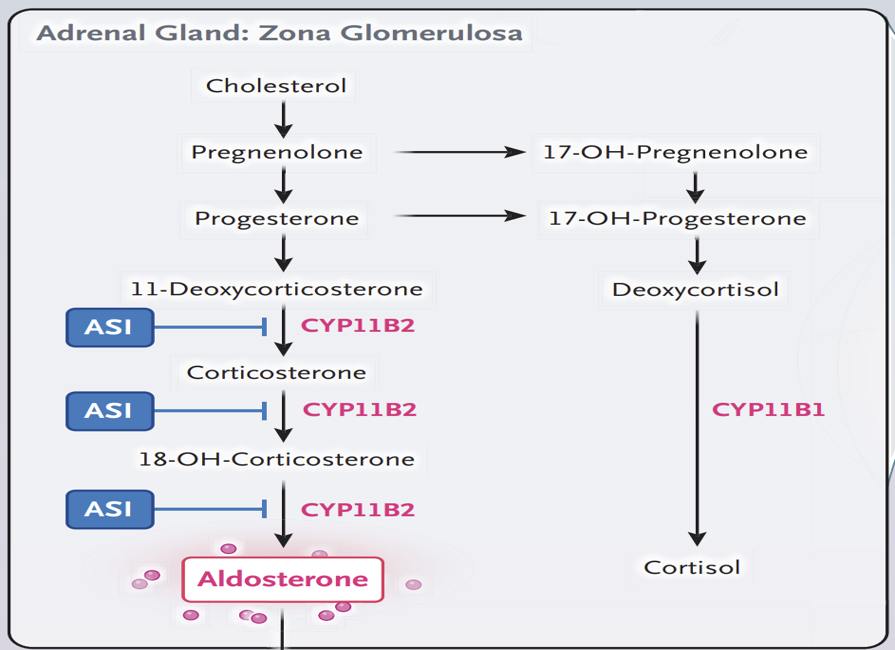
Adapted from Tomasz J et al NEJM Oct 2025
A number of Phase 3 randomised controlled trials have published demonstrating the efficacy and safety of baxdrostat in patients with uncontrolled or resistant hypertension. BaxHTN recruited patients with seated systolic BP of 140 – 170 mm Hg despite stable treatment with two antihypertensive medications (uncontrolled hypertension) or ≥ 3 anti-hypertensive medications including a diuretic (resistant hypertension) (5). 796 patients were randomised to either 1mg, 2mg baxdrostat once daily or placebo for 12 weeks.
At 12 weeks, the change from baseline in the least-squares mean seated systolic blood pressure was –14.5 mm Hg with 1-mg baxdrostat, –15.7 mm Hg with 2-mg baxdrostat, and –5.8 mm Hg with placebo. A potassium level of more than 6.0 mmol per liter was reported in 6 patients (2.3%) with 1-mg baxdrostat, in 8 patients (3.0%) with 2-mg baxdrostat, and in 1 patient (0.4%) with placebo. The authors noted reduced levels of aldosterone and increased levels of plasma renin activity that may suggest that baxdrostat may induce further urine sodium excretion in patients who are already being treated with diuretics, although this finding was not subject to hypothesis testing.
In the Bax24 trial, 854 patients with systolic BP 140-170 mmHg were similarly randomised to either 1mg, 2mg baxdrostat or placebo(6) . In this trial, the primary endpoint was change in 24 h ambulatory SBP. At 12 weeks, the change from baseline in the least-squares mean 24 h ambulatory SBP was –16·6 mm Hg in the baxdrostat group (n=89) and −2·6 mm Hg in the placebo group (n=95), The estimated placebo-corrected difference was −14·0 mm Hg. A confirmed potassium level of more than 6 mmol/L occurred in three (3%) of the 108 baxdrostat recipients and in none of the placebo recipients.
eGFR decreased by a mean of 8·7 (SD 14·0) mL/min per 1·73 m² during the trial, mainly within 2−4 weeks of baxdrostat treatment, but recovered towards baseline within 2 weeks after discontinuation of baxdrostat, consistent with a reversible functional eGFR change due to changes in renal perfusion pressure
Notably, the proportion of patients reaching 24h ambulatory SBP control (<130mmHg) was approximately 4 times higher with baxdrostat (71%) than placebo (17%). Over 12 weeks, baxdrostat lowered serum aldosterone concentrations by approximately 76% and increased plasma renin activity, findings consistent with inhibition of aldosterone synthase and the enhanced renal excretion of sodium.
In both trials, patients were already on at least 3 anti-hypertensives (including diuretics) and baxdrostat reduced systolic BP by a clinically meaningful level of between ~10-15mmHg. Both trials were over 12 weeks duration only with longer term data yet to come. Further, long-term renoprotection and cardio-protection trials are also on the way.
Baxdrostat have just been approved by the FDA in the US as the first and only aldosterone synthase inhibitor treatment for adults with hypertension. It is making its way to Australia as you read this article.
References:
- Caprio M, Feve B, Claes A, Viengchareun S, Lombes M, Zennaro MC. Pivotal role of the mineralocorticoid receptor in corticosteroid-induced adipogenesis. FASEB J. 2007;21:2185–94.
- Rondinone CM, Rodbard D, Baker ME. Aldosterone stimulated differentiation of mouse 3T3-L1 cells into adipocytes. Endocrinology. 1993;132(6):2421–6
- Ebata S, Muto S, Okada K, Nemoto J, Amemiya M, Saito T, Asano Y. Aldosterone activates Na+/H+ exchange in vascular smooth muscle cells by nongenomic and genomic mechanisms. Kidney Int. 1999;56(4):1400–12
- Leopold JA, Ingelfinger JR. Aldosterone and treatment-resistant hypertension. N Engl J Med 2023;388:464-7
- Flack JM, Azizi M, Brown JM, Dwyer JP, Jones ESW, Lihn AS, Liu L, Olsson DS, Perl S, Shibata H, Wang JG, Wilderäng U, Wittes JT, Williams B. Baxdrostat for uncontrolled and resistant hypertension: rationale and design of the Phase 3 clinical trials BaxHTN, BaxAsia, and Bax24. Hypertens Res. 2025 Nov;48(11):2911-2923.
- Azizi M, Brown JM, Dwyer JP, Flack JM, Jones ESW, Kurlyandskaya R, Li H, Birve F, Lihn AS, Perl S, Schlaich MP, Shibata H, Wang JG, Williams B; Bax24 investigators. Effect of baxdrostat on ambulatory blood pressure in patients with resistant hypertension (Bax24): a phase 3, randomised, double-blind, placebo-controlled trial. Lancet. 2026 Mar 7;407(10532):988-999.