
23rd May 2026, A/Prof Chee L Khoo

We all know about the causal association between the so called bad cholesterol, LDL-cholesterol (LDL-C) and atherosclerotic cardiovascular disease (ASCVD). There are suggestions that apolipoprotein B (apoB) levels might be a better reflection of atherosclerotic burden. There is now emerging consensus that relying on particle number whether with LDL-C or apoB is rather too simplistic. The cholesterol content of ApoB-containing particles varies considerably across individuals, generating cholesterol-depleted and cholesterol-enriched phenotypes (1,2).
ApoB is the main structural and singular nonexchangeable apolipoprotein on atherogenic lipoproteins. In addition to providing a scaffold for lipoproteins, it is also the principal ligand for the hepatic LDL receptor. Intestinal derived chylomicron particles and their remnants contain apoB-48 whereas hepatically derived VLDL, IDL, LDL-C and lipoprotein (a) contain apoB-100.
Routine diagnostic assays for apoB do not distinguish between apoB-48 and apoB-100; however, after a 12-hour fast under normal physiologic circumstances, it is mostly apoB-100 that is present in the circulation. Even postprandially, more than 95% of apoB in circulation is apoB-100 in individuals without severe hypertriglyceridemia (3). Therefore, there is minimal change in apoB levels in the fasting compared to the non-fasting state (4). Because there is a single apoB present on each atherogenic lipoprotein, the measured apoB level represents the serum concentration of atherogenic lipoproteins.
On a population level, LDL-C and apoB levels are fairly concordant. However, the lipid composition and size of LDL particles can vary greatly between individuals and even within an individual from one measurement to another (5,6). LDL-C can be measured by beta-quantification after ultra-centrifugation but it is cumbersome, time consuming and not readily available for clinical use.
What we see in our pathology reports are based on the Friedewald formula (total cholesterol – HDL – TG/2.2) in mmol/L. It actually calculate VLDL cholesterol based on the expected average of TG:cholesterol content in VLDL particles (7) but it becomes less reliable in patients with hypertriglycerides. There have been attempts to adjust for hypertriglyceridaemia with other formulae – Martin–Hopkins and Sampson-National Institutes of Health (NIH) equations (8,9). Non-HDL-C levels are used to avoid the “dilution” of total cholesterol affecting the LDL-C calculation.
ApoB assays
Commercial assays for apoB are based on either immunoturbidimetric or immune-nephelometric testing, which use antibodies that recognise both apoB-100 and apoB-48 and have been available for many years. It is highly accurate and reproducible. The cost of these assays is gradually coming down and may, one day be reimbursed under Medicare.
Which is better in predicting ASCVD risk?
Conditions such as hypertriglyceridemia, obesity, and insulin resistance can lead to smaller cholesterol-depleted LDL particles and result in lower LDL-C but still elevated apoB levels (10). This can lead to underestimation of CV risks and thence, undertreatment with lipid lowering therapy (LLT).
Even in patients with normal TG levels, there is a discordant between LDL-C and non-HDL-C but the discordance is less between apoB and non-HDL-C than the discordance between apoB and non-HDL-C. It has been consistently demonstrated that apoB and non-HDL-C are more closely associated with ASCVD risk than LDL-C, and apoB concentration predicts risk better than non-HDL-C (11-13).
How robust is data linking apoB levels and CV outcomes?
The data is actually limited. Randomised controlled trials (RCTs) investigating LLTs and cardiovascular outcomes have typically enrolled patients based on levels of cardiovascular risk and threshold LDL-C levels. Non-HDL-C and apoB have been measured or reported for some, but not all, of these trials. Some of these studies have reported effects of these therapies on LDL-C, non-HDL-C, and apoB levels along with cardiovascular outcomes (14-16). It is uncommon, though for LLT to have been adjusted during the RCTs based on achieved LDL-C levels and LLT were never adjusted based upon non-HDL-C or apoB concentrations. There are really no RCTs conducted in which participants at risk of ASCVD were randomised to treatment strategies based on achieving non-HDL-C or apoB therapeutic targets to determine which strategy results in the best cardiovascular outcomes.
Nonetheless, in the Scandinavian Simvastatin Survival Study (4S), there was a 1% reduction resulted in a decrease of major coronary events of 1.7% for LDL-C, 1.7% for non-HDL-C, and 1.1% for apoB (17). In the Incremental Decrease in End Points Through Aggressive Lipid Lowering (IDEAL) trial, both non-HDL-C and apoB changes were better predictors of coronary events than LDL-C in an analysis (18). The Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) and Pravastatin or Atorvastatin Evaluation and Infection Therapy–Thrombolysis in Myocardial Infarction 22 (PROVE-IT TIMI22) trials found that on-treatment LDL-C, non-HDL-C, and apoB were similarly predictive of subsequent cardiovascular events (19,20).
In the Evaluation of Cardiovascular Outcomes After an Acute Coronary Syndrome During Treatment with Alirocumab (ODYSSEY OUTCOMES) where alirocumab or placebo were added to maximally tolerated statin, CV outcomes were increased with increasing apoB levels after adjusting for baseline LDL-C (21). Using the combined datasets from the FOURIER (using evolocumab) and IMPROVE-IT (using simvastatin) trials, apoB was the best predictor of myocardial infarction risk and that it remained predictive even when adjusted for non-HDL-C and triglyceride concentrations (22).
So, what apoB treatment targets should we use?
Because we don’t have data from specific RCT using apo levels as a treatment, there are no specific apoB thresholds in U.S. or international guidelines and recommendations. Suggested apoB thresholds are listed in Table 4.
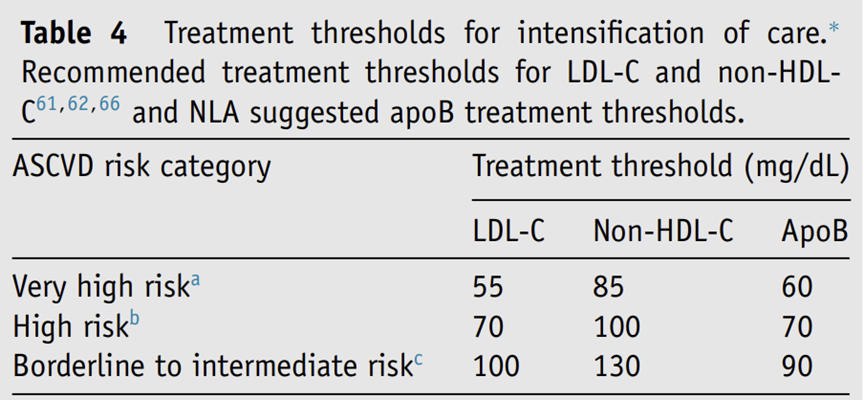
Adapted from Soffer D, et al Journal of Clinical Lipidology Sept/Oct 2024
Wang et al recent hypothesised that in patients without apoB measured, LDL-C/TC ratios might be a superior ASCVD risk marker than calculated LDL-C or non-HDL-C levels. A ratio ≥0.60 identifies individuals whose atherogenic risk may be underestimated by LDL-C, non–HDL-C, triglycerides, or CV risk calculator –based risk scores.
In patients where apoB levels are available, and when ApoB and the LDL-C/TC ratio were considered together, four distinct lipid profiles showed clear risk separation: people with both markers in the normal range had the lowest long-term risk, while those with both elevated had the highest risk. Importantly, a high LDL-C/TC ratio identified a higher-risk group even among individuals with normal ApoB, which may be overlooked in routine care.
Be wary of the calculated LDL-C especially in patients with high triglyceridaemia when assessing the cardiovascular risk of the patient sitting in front of you. You should use the non-HDL-C which is a better marker of CV risks. Now, you may want to use the LDL-C/TC ratio until we have easy access to apoB testing.
References:
- Marston NA, Giugliano RP, Melloni GEM, et al. Association of Apolipoprotein B Containing Lipoproteins and Risk of Myocardial Infarction in Individuals With and Without Atherosclerosis: Distinguishing Between Particle Concentration, Type, and Content. JAMA Cardiol 2022;7:250-256.
- Sniderman AD, Navar AM, Thanassoulis G. Apolipoprotein B vs Low-Density 2 Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as the Primary Measure 3 of Apolipoprotein B Lipoprotein-Related Risk: The Debate Is Over. JAMA Cardiol 2022;7:257- 4 258
- Glavinovic T, Thanassoulis G, de Graaf J, Couture P, Hegele RA, Sniderman AD. Physiological bases for the superiority of apolipoprotein B over low-density lipoprotein cholesterol and non-high-density lipoprotein cholesterol as a marker of cardiovascular risk. J Am Heart Assoc. 2022;11(20):e025858. doi:10.1161/JAHA.122.025858. 5.
- Otokozawa S, Ai M, Diffenderfer MR, et al. Fasting and postprandial apolipoprotein B-48 levels in healthy, obese, and hyperlipidemic subjects. Metabolism. 2009;58(11):1536–1542. doi:10.1016/j.metabol. 2009.04.040
- Havel RJ, Eder HA, Bragdon JH. The distribution and chemical com[1]position of ultracentrifugally separated lipoproteins in human serum. J Clin Invest. 1955;34(9):1345–1353. doi:10.1172/JCI103182.
- Sniderman AD, Dufresne L, Pencina KM, Bilgic S, Thanassoulis G, Pencina MJ. Discordance among apoB, non-high-density lipoprotein cholesterol, and triglycerides: implications for cardiovascular prevention. Eur Heart J. 2024.
- Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18(6):499–502.
- Martin SS, Blaha MJ, Elshazly MB, et al. Comparison of a novel method vs. the Friedewald equation for estimating low-density lipoprotein cholesterol levels from the standard lipid profile. JAMA. 2013;310(19):2061–2068
- Sampson M, Ling C, Sun Q, et al. A new equation for calculation of low density lipoprotein cholesterol in patients with normolipidemia and/or hypertriglyceridemia. JAMA Cardiol. 2020;5(5):540–548.
- Wilkins JT, Li RC, Sniderman A, Chan C, DM Lloyd-Jones. Discordance between apolipoprotein B and LDL-cholesterol in young adults predicts coronary artery calcification: the CARDIA study. J Am Coll Cardiol. 2016;67(2):193–201
- Sniderman AD, Dufresne L, Pencina KM, Bilgic S, Thanassoulis G, Pencina MJ. Discordance among apoB, non-high-density lipoprotein cholesterol, and triglycerides: implications for cardiovascular prevention. Eur Heart J. 2024
- Lawler PR, Akinkuolie AO, Ridker PM, et al. Discordance between circulating atherogenic cholesterol mass and lipoprotein particle concentration in relation to future coronary events in women. Clin Chem. 2017;63(4):870–879
- Johannesen CDL, Mortensen MB, Langsted A, Nordestgaard BG. Apolipoprotein B and non-HDL cholesterol better reflect residual risk than LDL cholesterol in statin-treated patients. J Am Coll Cardiol. 2021;77(11):1439–1450
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372(25):2387–2397.
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722.
- Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379(22):2097–2107
- Pedersen TR, Olsson AG, Faergeman O, et al. Lipoprotein changes and reduction in the incidence of major coronary heart disease events in the scandinavian simvastatin survival study (4S). Circulation. 1998;97(15):1453–1460.
- Holme I, Cater NB, Faergeman O, et al. Lipoprotein predictors of car[1]diovascular events in statin-treated patients with coronary heart disease. Insights from the incremental decrease in end-points through aggressive lipid-lowering trial (IDEAL). Ann Med. 2008;40(6):456–464.
- Mora S, Glynn RJ, Boekholdt SM, Nordestgaard BG, Kastelein JJ, Ridker PM. On-treatment non-high-density lipoprotein cholesterol, apolipoprotein B, triglycerides, and lipid ratios in relation to residual vascular risk after treatment with potent statin therapy: JUPITER (justification for the use of statins in prevention: an intervention trial evaluating rosuvastatin). J Am Coll Cardiol. 2012;59(17):1521–1528.
- Ray KK, Cannon CP, Cairns R, Morrow DA, Ridker PM, Braunwald E. Prognostic utility of apoB/AI, total cholesterol/HDL, non-HDL cholesterol, or hs-CRP as predictors of clinical risk in patients receiving statin therapy after acute coronary syndromes: results from PROVE IT-TIMI 22. Arterioscler Thromb Vasc Biol. 2009;29(3):424–430
- Hagstrom E, Steg PG, Szarek M, et al. Apolipoprotein B, residual cardiovascular risk after acute coronary syndrome, and effects of alirocumab. Circulation. 2022;146(9):657–672
- Marston NA, Giugliano RP, Melloni GEM, et al. Association of apolipoprotein B-containing lipoproteins and risk of myocardial infarction in individuals with and without atherosclerosis: distinguish[1]ing between particle concentration, type, and content. JAMA Cardiol. 2022;7(3):250–256.
- Daniel E. Soffer, Nicholas A. Marston, Kevin C. Maki, et al. Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: An Expert Clinical Consensus from the National Lipid Association Journal of Clinical Lipidology, Vol 18, No 5, September/October 2024
- Wang B, Nurmohamed NS, Kraaijenhof JM, Li D. ASCVD Risk Stratification Using Apolipoprotein B and the LDL-C to Total Cholesterol Ratio. Eur J Prev Cardiol. 2026 May 9:zwag260.